

Abstract
Introduction: In the prospective, multicenter AML-BFM 98 study for children and adolescents with acute myeloid leukemia (AML), it was randomly tested whether granulocyte colony-stimulating factor (G-CSF) can reduce infectious complications and improve outcome (161 patients with G-CSF, 156 without G-CSF). G-CSF administration did not result in less morbidity or mortality and higher event-free survival (EFS) (Lehrnbecher et al. Blood 2007). Subgroup analysis suggested an increased number of relapses in the standard risk (SR) group (i.e. AML FAB1/2 with Auer rods, FAB M4eo, AML with t(8;21) or inv16: if less than 5% of blasts on day 15) after G-CSF treatment (p=0.06). Relapses of SR patients did not correlate with initial leukocyte count, age, FAB subtype or cytogenetic aberrations.
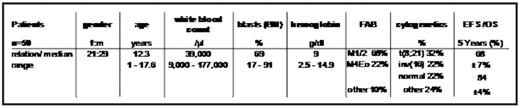
Patients/Methods: We analyzed 50 SR patients (of n=162 SR patients in trial ALM-BFM 98) for G-CSF receptor (G-CSFR) expression. Surface expression of the G-CSFR was measured by immunophenotyping, and G-CSFR RNA isoform I and IV were analysed with real-time quantitative RT-PCR (RQ-RT-PCR). G-CSFR isoform IV overexpression was defined as expression higher than the median G-CSFR isoform IV expression in all analyzed SR patients. Minimal residual disease (MRD) was monitored by immunophenotyping and, if cytogenetic aberrations were detectable, by RQ-RT-PCR (Langebrake et al. JCO 2006; Viehmann et al. Leukemia 2003). All patients were screened for acquired mutations of the cytosolic domain of the G-CSFR by direct sequencing and subcloning.
Results: G-CSFR surface expression and MRD monitoring revealed no correlation with the risk of relapse. Notably, we found that even in complete morphologic remission after 1st and 2nd induction, there were still low numbers of blasts in nearly all patients. No G-CSFR mutations–as common in congenital neutropenia-were identified in this patient group.
In patients randomized to receive G-CSF after induction, the 16 patients overexpressing the differentiation-defective G-CSFR isoform IV showed an increased 5-year cumulative incidence of relapse (CI 50±13 %) as opposed to the 14 patients with low expression (CI of 14±10 %; p log rank=0.04). In patients not receiving G-CSF, the level of G-CSFR isoform IV had no significant influence on CI (0±0 % in patients with high expression (n=9), and 82±12 % in patients with low expression (n=11), p=0.19.
Multivariate analyses including G-CSFR isoform IV overexpression, sex and favourable cytogenetics within the G-CSF-treated subgroup revealed prognostic relevance of G-CSFR isoform IV overexpression for EFS (p=0.031) and CI (p=0.049).
Conclusion: Our results demonstrate that children and adolescents with an AML overexpressing the differentiation-defective G-CSFR isoform IV respond to G-CSF administration after induction with significantly higher number of relapses. AML with overexpression of the differentiation-defective G-CSFR isoform IV should not be treated with G-CSF.
Disclosures: No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal