Introduction. Hypomethylating agents azacitidine (AZA) and decitabine are standard of care for myelodysplastic syndromes (MDS). Considering the result of the secondary analysis of the AZA-001 trial showing 91% of first responses occurred within 6 cycles, the concept is widely accepted that AZA should be performed at least 6 cycles even if early response is not achieved (Silverman LR, Cancer. 2011). However, 40-50% of cases finally experienced primary resistance. These facts mean almost half of the patients receive fruitless treatment for up to six months. Therefore, it is necessary to identify those patients who do not response to AZA from the early cycles, so that they can receive alternative treatment as early as possible.
The Wilms' tumor 1 gene (WT1) is a tumor marker of leukemic blasts. High expression of WT1-mRNA is correlated with disease progression, efficacy of AZA and prognosis in the patients with MDS (Tamaki et al, Leukemia. 1999). In this study, we explored whether WT1-mRNA levels in peripheral blood (PB) samples at baseline and during the early cycles of AZA could be useful in predicting outcome to this therapy.
Methods. We retrospectively evaluated transplant-ineligible patients with high-risk MDS, diagnosed according to the 2008 World Health Organization classification, who received more than three cycles of AZA as a 1st line therapy between March 2012 and January 2020 at Aiiku Hospital and Sapporo Hokuyu Hospital. Response to treatment was classified as complete remission (CR), partial remission (PR), hematologic improvement (HI), stable disease, and failure based on the International Working Group 2006 criteria. Patients who were not evaluated WT1-mRNA levels in PB samples at baseline and within three cycles of AZA were excluded from this study. WT1-mRNA was measured using a WT1-mRNA Assay Kit (Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan). The study procedures were in accordance with the Helsinki Declaration and institutional ethical guidelines, and were approved by the institutional review boards.
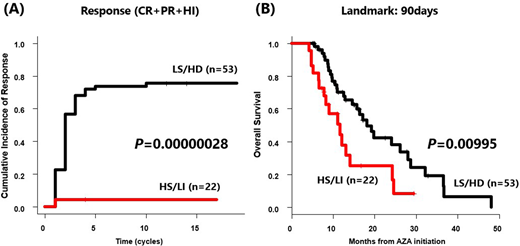
Results. Seventy-five patients (age 61-88, median 77; 76% male) were included in this study. The median follow-up time from AZA initiation was 11.4 months (range, 4.2-48.8 months). Median overall survival (OS) time from AZA initiation was 16.4 months (95% CI, 11.6-24.1 months). Forty-one patients (54.7%) achieved any response (CR + PR + HI). WT1-mRNA expression at the baseline varied from <50 to 320000 copies/µg RNA (median, 3400 copies/µg RNA). We classified them into four groups based on the dynamics of PB WT1-mRNA levels within three cycles of AZA, with a threshold of the median level for the definition of "high" or "low" WT1-mRNA levels. Low-increase (LI) group included patients with low WT1-mRNA level at baseline and elevated to high level with 2 times or more than the baseline. Low-stable (LS) group included cases with initial WT1-mRNA level low but did not meet the LI criteria. High-decrease (HD) group included patients with initial WT1-mRNA level high and decreased to less than half of it. High-stable (HS) group included cases with initial WT1-mRNA level high but did not meet the HD criteria. Six patients were included in the LI, 32 patients in LS, 21 patients in HD, and 16 patients in HS. The median number of AZA cycles in LS/HD was 11 (range, 3-34 cycles), while in HS/LI was 7 (range, 3-17 cycles). Cumulative incidence of any response after 10 cycles of AZA was significantly higher in LS/HD than in HS/LI (75.5% vs 4.5%, P=0.00000028; Gray test, Figure A). For LS/HD, the median OS was 18.2 months (95% CI, 12.8-28.1 months), whereas HS/LI had a median OS of 11.6 months (95% CI, 6.6-14.1 months; P=0.00995; Log-rank, Figure B). A multivariate analysis demonstrated that Poor/Very poor International Prognostic Scoring System (IPSS-R) cytogenetic risk and HS/LI were independently associated with poor outcome (OS; Poor/Very poor IPSS-R cytogenetic risk; HR, 2.33; 95% CI, 1.24 to 4.38, P=0.0087, HS/LI; HR, 2.46; 95% CI, 1.31 to 4.61, P=0.0052; Cox regression analysis). Altogether, we demonstrated that dynamic change of PB WT1-mRNA within three cycles of AZA predicts response for AZA and prognosis in patients with high-risk MDS.
Conclusion. Dynamic change of PB WT1-mRNA within three cycles of AZA was correlated with response for AZA in patients with high-risk MDS. Moreover, patients in HS/LI could not get any further response by continuous cycles of AZA and should be considered for alternative options.
Teshima:Takeda Pharmaceutical Company Limited: Consultancy, Honoraria; Kyowa Kirin Co., Ltd.: Honoraria, Research Funding; Merck: Consultancy, Honoraria; Sharp & Dohme Corp: Consultancy, Honoraria; Sanofi K.K.: Research Funding; TEIJIN PHARMA LIMITED: Honoraria; Chugai Pharmaceutical Co., Ltd.: Research Funding; Astellas Pharma Inc.: Research Funding; The Center of Innovation Program from Japan Science and Technology Agency: Other; Japan Society for the Promotion of Science KAKENHI (17H04206): Other; Janssen Pharmaceutical K.K.: Other; NIPPON SHINYAKU CO., LTD.: Honoraria; Fuji Pharma Co., Ltd.: Honoraria; Novartis Pharma K.K.: Consultancy, Other: Manuscript preparation, Research Funding; Bristol-Myers Squibb: Honoraria; Pfizer Japan Inc.: Honoraria.