Key Points
Using a systematic approach, we identified 23 prognostic factors for venous thromboembolism and 15 for bleeding.
We identified several prognostic factors for VTE and bleeding that are not considered in most of the widely used risk assessment models.

Abstract
There may be many predictors of venous thromboembolism (VTE) and bleeding in hospitalized medical patients, but until now, systematic reviews and assessments of the certainty of the evidence have not been published. We conducted a systematic review to identify prognostic factors for VTE and bleeding in hospitalized medical patients and searched Medline and EMBASE from inception through May 2018. We considered studies that identified potential prognostic factors for VTE and bleeding in hospitalized adult medical patients. Reviewers extracted data in duplicate and independently and assessed the certainty of the evidence using the Grading of Recommendations Assessment, Development, and Evaluation approach. Of 69 410 citations, we included 17 studies in our analysis: 14 that reported on VTE, and 3 that reported on bleeding. For VTE, moderate-certainty evidence showed a probable association with older age; elevated C-reactive protein (CRP), D-dimer, and fibrinogen levels; tachycardia; thrombocytosis; leukocytosis; fever; leg edema; lower Barthel Index (BI) score; immobility; paresis; previous history of VTE; thrombophilia; malignancy; critical illness; and infections. For bleeding, moderate-certainty evidence showed a probable association with older age, sex, anemia, obesity, low hemoglobin, gastroduodenal ulcers, rehospitalization, critical illness, thrombocytopenia, blood dyscrasias, hepatic disease, renal failure, antithrombotic medication, and presence of a central venous catheter. Elevated CRP, a lower BI, a history of malignancy, and elevated heart rate are not included in most VTE risk assessment models. This study informs risk prediction in the management of hospitalized medical patients for VTE and bleeding; it also informs guidelines for VTE prevention and future research.
Introduction
Venous thromboembolism (VTE), comprising deep vein thrombosis (DVT) and pulmonary embolism (PE), has an annual incidence of ∼1 per 1000 in adult populations.1,2 VTE is a major burden in hospitalized medical patients. Medical patients can be classified as having acute, critical, or chronic medical illness, and their risk for both VTE and bleeding may depend on the severity of their medical illness. The incidence of VTE in hospitalized acutely ill medical patients detected by screening is up to 14.9%.3 From 50% to 70% of symptomatic VTEs and 70% to 80% of fatal PEs occur in acute medically ill patients.4-7
The risk of hospital-acquired VTE is reduced by using pharmacological and nonpharmacological interventions, but these interventions are not without potential patient harms. Risk assessment models (RAMs) have been used in hospitalized medically ill patients to stratify the different subsets of patients by their risk of having a VTE or clinically significant bleeding event.8 This stratification may then support optimized management for the prevention of either outcome.9 A RAM is a formal combination of multiple predictors from which risks of a specific end point can be calculated for individuals. The value of using RAMs include generation of specific baseline risks to inform recommendations for a strata of patients and calculation of a predicted risk of an outcome for an individual patient (eg, VTE or bleeding) based on the patient’s characteristics (ie, the prognostic factors). Implementation of RAMs in the field of VTE prevention can be accomplished by embedding them in clinical encounters or decision aids to individualize the use of guideline recommendations. However, the application of RAMs is variable in current practice.3
Most RAMs are developed using data registries that are not based on a systematic review of all potential prognostic factors.10 However, guiding principles for developing RAMs describe the importance of identifying prognostic factors through systematic reviews.10 We identified only one systematic review, conducted 11 years ago, that evaluated VTE as an outcome in medical patients, but the effect sizes of the prognostic factors were not subjected to meta-analysis, and bleeding risk, critical for balancing benefits and harms in these patients, was not included as an outcome.11
Therefore, our aim was to conduct a systematic review of prognostic factors for VTE and bleeding in hospitalized medical patients that may inform management, future guideline recommendations, and the development of RAMs in hospitalized medical patients.
Methods
We conducted a systematic review using Cochrane methodology to identify studies that reported on prognostic factors for VTE and bleeding in hospitalized medical patients.12 We developed a protocol that was reviewed and revised by the coauthors, but we did not register it because of confidentiality clauses in the research contract.
Data sources and searches
We searched Medline and EMBASE from inception through May 2018 with the assistance of an information scientist. Supplemental Table 1 (available on the Blood Web site) provides detailed descriptions of the search strategy. The search included both medical subject heading (MesH) terms and text-word terms. It combined VTE-related terms with primary prevention terms and 2 search blocks defining prognosis and prediction guide filters. We used no language restrictions or time limits.
Study selection
Four teams of 2 reviewers participated in training and calibration exercises before starting the screening processes. The teams screened independently and in duplicate the titles and abstracts of all the retrieved citations. They then retrieved the full texts of all citations judged as potentially eligible by at least 1 of the reviewers on each team. The reviewers screened the full texts independently and in duplicate and compared their results. A third senior reviewer resolved disagreements when necessary. Reviewers used a standardized screening form and conducted calibration exercises before the screening process. The eligibility criteria for study selection comprised the following characteristics.
Population
We included studies that evaluated adult medical patients who were acutely, critically, or chronically ill. We also included studies in which the population included nonmedical patients or medical patients with a recent history of surgery or trauma if the final regression model adjusted for these factors. We included studies if less than 10% of the population was receiving thromboprophylaxis or if the statistical analysis adjusted for the use of thromboprophylaxis. Thromboprophylaxis included the use of anticoagulation therapy (ie, warfarin, low-molecular-weight heparin, and unfractionated heparin), antiplatelet therapy (ie, aspirin), or mechanical prophylaxis (ie, elastic stockings or intermittent pneumatic compression).
We excluded studies if the population did not reflect the general population of interest, such as studies of only selected types of cancer patients.13,14 We defined acutely ill medical patients as those hospitalized for a medical illness including heart failure, respiratory insufficiency, stroke, and infectious or inflammatory diseases requiring urgent care.2 Critically ill patients were those who had an immediately life-threatening condition and were admitted to an intensive or critical care unit.2 Chronically ill medical patients included those with acute exacerbations of chronic medical conditions who required hospitalization.2
Exposure
We investigated all prognostic factors reported in individual studies.
Comparisons
We investigated the absence or different levels of the prognostic factor.
Outcomes
Studies had to report on the outcomes VTE or bleeding. VTE was defined as any symptomatic or asymptomatic DVT or PE within 90 days after discharge. Bleeding included major or nonmajor but clinically significant bleeding within 90 days after discharge.8
Setting
Studies that included patients who were admitted to a nonsurgical inpatient ward.
Type of study
Data extraction
Two reviewers abstracted data independently and in duplicate from all eligible studies using standardized forms. Reviewers compared and discussed results and consulted a third reviewer in case of any disagreement. We conducted calibration exercises and piloting of all forms before the start of the data abstraction process. All eligible studies were published in English.
For all identified studies, RAMs, and prognostic factor studies, the reviewers abstracted data on the following characteristics:
Study context (eg, country and year of publication)
Type of prediction model study (development, validation, and impact)
Study design (eg, cohort or case-control; duration of follow-up)
Population and their demographics (eg, sample size, age, number of centers, and administration of prophylaxis and what type)
Outcomes (VTE and bleeding)
Prognostic factors, definitions, and measurement methods (including thresholds used for continuous predictors)
Measures of association (eg, odds ratio [OR], risk ratio, and hazard ratio)
Quality assessment
Risk-of-bias assessment
Synthesis of findings and certainty of evidence assessment
We presented the results of the studies, including the individual prognostic factors, in both tabular and narrative formats. We also described the identified prognostic factor studies and the measure of association with the outcomes of interest. We performed an assessment of the certainty of evidence for each of the prognostic factors per outcome, based on the GRADE approach.15 The approach considers the following domains: risk of bias, indirectness, inconsistency, imprecision, and publication bias. We developed evidence profiles and rated the overall certainty of evidence as high, moderate, and low or very low, depending on the grading of the individual domains.15 We narratively described the strength of the association using the terms “there is,” “there probably is,” or “there may be,” depending on whether the quality of the evidence was “high,” “moderate,” or “low/very low,” respectively.
Data synthesis and analysis
We standardized the units of measurement for each prognostic factor, unifying the direction of the predictors, adjusting the weights of the studies, and calculating crude-effect estimates when not provided.21 When possible, we performed meta-analysis of all prognostic factors associated with the outcomes VTE and bleeding that were reported by more than 1 study. We then presented the effect estimate as OR and the corresponding 95% confidence interval (CI). In studies that reported the measure of association as an hazard ratio or risk ratio, we converted them to ORs using the baseline risk (incidence of those not on prophylaxis having VTE or bleeding out of the total sample) reported in the studies.22,23 We conducted a meta-analysis of associations using the generic inverse variance-based method to produce an overall measure of association. We used the crude effect estimates when the adjusted estimates were not provided. We explored consistency of the associations between the results of our meta-analysis and studies reporting the same predictors that could not be pooled. All analyses used random-effect models applying the prognosis module in Review Manager, version 5.3.24
Results
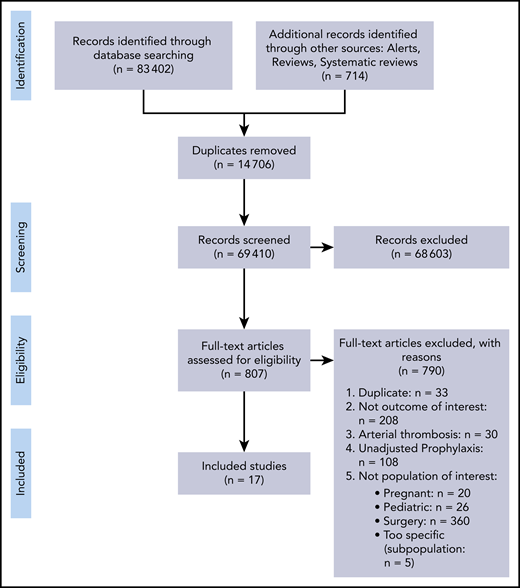
Figure 1 is a Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart. Our search identified 69 410 citations, of which we included 807 studies for full text assessment. Seventeen studies fulfilled the inclusion criteria for evaluating VTE or bleeding outcomes or both.7,8,25-39

Description of included studies
Table 1 describes the characteristics of the included studies reporting on the outcomes VTE and/or bleeding. Eight studies were prognostic factor studies: 4 were prognostic model development studies, and 5 were external validation studies. Five studies were retrospective case-control studies,25-29 2 of which were multicenter25,26 ; 5 were retrospective cohorts,30-34 3 of which were multicenter.31,32,34 Seven studies were prospective cohorts,7,8,35-39 4 of which were multicenter.7,8,36,39 The included studies were conducted in the United States (n = 9), China (n = 3), Canada (n = 2), United Kingdom (n = 1), Poland (n = 1), and Japan (n = 1). Of the 14 included studies for VTE (defined as proximal DVT or PE), 9 reported on symptomatic VTE only.7,25-31,34 The other 5 studies reported on both symptomatic and asymptomatic VTE.35-39 The follow-up time was up to 3 months in 12 of 14 studies reporting on VTE. The other 2 studies, Zhou et al29 and Yi et al,39 had a follow-up time of 6 months and 1 year, respectively, but also reported the occurrence of VTE during hospitalization. In accordance with our protocol, we used the incidence of VTE during hospitalization from those studies. The 3 studies that reported on bleeding (major or clinically relevant) had a follow-up time up to 1 month.8,32,33 Of the 14 studies reporting on VTE, 12 studies included patients who received thromboprophylaxis in 0.4% to 67% of the patients. Of those, 2 studies35,36 included less than 10% of patients on thromboprophylaxis, and 10 studies adjusted for prophylaxis in the statistical analysis.7,26-31,34,38,39 As for bleeding, all 3 studies reported prophylaxis use in 9% to 70%, which was accounted for in their analysis.8,32,33
Risk-of-bias assessment
Risk of bias was serious across all identified studies, each presenting risk of bias in at least 1 domain or item (Tables 2 and 3). Among the 17 included studies, 10 were retrospective, which may have introduced classification bias.25-34 Seven of the 8 prognostic factor studies included only the variables significant in bivariable analysis in their final regression model and did not present any data for nonsignificant predictors in their adjusted analysis.30,32,33,36-39 Two of the 8 prognostic factor studies32,33 and 4 of the 9 prognostic model development or validation studies did not have a clear description of appropriate outcome measurement.26-29 We detected no evidence of publication bias through visual assessment of asymmetry of the funnel plot for each pooled predictor in those that included at least 10 studies (Tables 2 and 3). Supplemental Table 2 provides the detailed judgements for each of the risk-of-bias domain criteria.
Prognostic factors for VTE in hospitalized medical patients
Investigated were 29 candidate prognostic factors for VTE from 14 studies including 15 1 714 patients. Table 2 provides the evidence profile for VTE-related prognostic factors. Supplemental Figure 1 provides the forest plots of the meta-analysis of each of the prognostic factors.
Demographic factors
We found moderate-certainty evidence that there is probably an association between risk of any VTE and age ≥60 y (OR, 1.34; 95% CI, 1.17-1.55),7,25-27,29,31,34-37,39 and that there is probably little to no association between risk of any VTE and sex (males vs females: OR, 1.03; 95% CI, 0.80-1.33).27,34-37
Functional factors
There was moderate-certainty evidence for a probable association between risk of any VTE and lower Barthel Index scores (BI ≤ 9; OR, 8.30; 95% CI, 2.70-25.52)37 ; immobility, defined as confinement to bed for >72 hours or >7 days or bedridden or nonambulatory (OR, 3.17; 95% CI, 2.18-4.62)7,25,26,28,29,31,37,39 ; and paresis (OR, 2.97; 95% CI, 1.20-7.36).7,25,26,37
Medical illness and patient history factors
We identified moderate-certainty evidence for an association between risk of any VTE and history of VTE (OR, 6.08; 95% CI, 3.71-9.97)7,25-27,29-31,36 ; thrombophilia, defined as familial or acquired disorder of the hemostatic system (OR, 5.88; 95% CI, 2.80-12.35)7,25,26,29,34 ; history of malignancy (OR, 3.20; 95% CI, 2.14-4.79)27 ; active malignancy defined as the presence of cancer on admission or within the past year (OR, 2.65; 95% CI, 1.79-3.91)7,25,27,28,30,31,34,36,37 ; critical illness, defined as intensive care unit (ICU) or coronary care unit (CCU) stay or need for resuscitation (OR, 1.65; 95% CI, 1.39-1.95)7,25-27,29,34,36 ; and infections including cellulitis, pneumonia, and sepsis (OR, 1.48; 95% CI, 1.16-1.89).27-29,31,36
We found low-certainty evidence that there may be an association between risk of any VTE and history of heart failure (OR, of 2.68; 95% CI, 1.11-6.44)27,29,35 ; autoimmune diseases, including rheumatological diseases and inflammatory diseases (OR, 2.33; 95% CI, 1.13-4.83)31,34,36,39 ; central venous catheter (CVC) use (OR, 2.05; 95% CI, 0.74-5.65)31,34 ; and severe stroke, defined as acute ischemic stroke (OR, 1.79; 95% CI, 0.77-4.18).29,31,32,35,36 The findings for severe stroke when assessed using a diagnostic tool, the National Institutes of Health Stroke Scale (NIHSS), were consistent with our results (Table 2).35 We also identified low-certainty evidence that there may be an association between risk of any VTE and current tobacco use (OR, 1.59; 95% CI, 0.28-9.03); however, there may be little to no association between risk of any VTE and previous tobacco use (OR, 0.97; 95% CI, 0.24-3.92).
Furthermore, we identified low-certainty evidence that there may be little to no association between the risk of any VTE and respiratory failure (OR, 1.04; 95% CI, 0.69-1.58), coronary artery disease (CAD; OR, 1.01; 95% CI, 0.33-3.09), acute heart failure (OR, 0.82; 95% CI, 0.42-1.60),31,36 and hormone use (OR, 0.8; 95% CI, 0.36-1.78).29,31,36,37
We found very-low-certainty evidence that there may be little to no association between risk of any VTE and chronic renal failure (OR, 0.76; 95% CI, 0.18-3.18).36
Laboratory and physical examination factors
There is moderate-certainty evidence of an association between risk of any VTE and C-reactive protein (CRP) >10 mg/L (OR, 10.10; 95% CI, 1.93-52.85)35 and D-dimer >500 ng/mL at baseline (OR, 2.46; 95% CI, 1.19-5.10).36 The findings for D-dimer concentration, when assessed as a continuous variable, were consistent with our results (Table 2).39 Also, there is probably an association between risk of any VTE and elevated heart rate (>100 beats per minute; OR, 2.48; 95% CI, 1.66-3.71),27 thrombocytosis (platelet count, >350 × 109/L; OR, 2.16; 95% CI, 1.40-3.35),27,28 leukocytosis (white blood cell count, ≥11 × 109/L; OR, 1.91; 95% CI: 1.24-2.94),27 fever (body temperature >38°C-38.5°C; OR, 1.88; 95% CI, 1.10-3.21),27,28 leg edema (OR, 1.88; 95% CI, 1.23-2.90),28,31 and elevated fibrinogen level (>400 mg/dL; OR, 0.18; 95% CI, 0.04-0.81).35
We identified low-certainty evidence that there may be an association between risk of any VTE and varicose veins (OR, 1.53; 95% CI, 0.85-2.76)29,31 and obesity (BMI >30 kg/m2; OR, 1.34; 95% CI, 0.94-1.91).27,29,31,34,36
Additional analyses
We performed a sensitivity analysis, including studies that reported on immobility, to compare the association between immobility >72 hours and >7 days with risk of VTE. We found similar effect estimates for both categories with a slightly stronger association between immobility, defined as bed rest for >7 days, and risk of VTE (OR, 3.67; 95% CI, 0.85-15.93) compared with immobility, defined as bed rest for >72 hours, and risk of VTE (OR, 3.18; 95% CI, 1.10-9.16).
We also conducted a sensitivity analysis, including studies that reported on symptomatic VTE only, to evaluate the influence of the studies that reported on both symptomatic and asymptomatic VTE. The results of the sensitivity analysis showed similar effect estimates across prognostic factors except for CAD. The association between CAD and risk of symptomatic VTE was somewhat stronger in the sensitivity analysis of the 9 studies (OR, 2.02; 95% CI, 0.32-12.64), compared with little to no association with risk of VTE in the primary analysis (OR, 1.01; 95% CI, 0.33-3.09; supplemental Table 4).
Prognostic factors for bleeding in medical hospitalized patients
Three studies including 160 142 patients investigated 17 candidate prognostic factors for bleeding. Table 3 provides the evidence profile for bleeding-related prognostic factors. Supplemental Figure 2 provides the forest plots of the meta-analyses of each of the prognostic factors.
Demographic factors
Medical illness and patient history factors
There was moderate-certainty evidence of a probable association between risk of bleeding and gastroduodenal ulcers (OR, 2.74; 95% CI, 1.42-5.26),8,32 rehospitalization (OR, 2.39; 95% CI, 2.25- 2.54),32 critical illness including ICU or CCU stay (OR, 2.10; 95% CI, 1.42-3.11),8 and thrombocytopenia (OR, 1.79; 95% CI 0.97-3.29).8,32,33 When cutoffs for thrombocytopenia were assessed separately, results showed that there probably is a greater magnitude of association between risk of bleeding and platelet count <50 × 109/L compared with a platelet count ≥50 × 109/L (OR, 3.37; 95% CI, 1.84-6.18),26 whereas a smaller magnitude of association between risk of bleeding and platelet count <150 × 109/L compared with platelet count ≥150 × 109/L (OR, 1.30; 95% CI, 0.92-1.82).30,32 We also found moderate-certainty evidence that there is probably an association between risk of bleeding and blood dyscrasia, defined as the presence of any bleeding disorder on admission (OR, 1.70; 95% CI, 1.60-1.81),32 hepatic disease (OR, 1.53; 95% CI, 1.09-2.15),8,32 and renal failure (OR, 1.43; 95% CI, 1.06-1.93).8,32 One study assessed renal failure by severity and the results showed that there probably is a greater magnitude of association between risk of bleeding and severe renal failure (glomerular filtration rate [GFR] <30 mL/min/m2) vs no severe renal failure (OR, 2.14; 95% CI, 1.22-3.75)8 and a smaller magnitude of association between risk of bleeding and moderate renal failure (GFR, 30-59 mL/min/m2) compared with no moderate renal failure (OR, 1.37; 95% CI, 0.84-2.23).8 We also identified moderate-certainty evidence that there is probably an association between risk of bleeding and CVC use (OR, 1.37; 95% CI, 0.83-2.26)8,32 and antithrombotic medication use (OR, 1.28; 95% CI, 1.01-1.64).8,32
We found moderate-certainty evidence that there is probably little to no association between risk of bleeding and hormone use, defined as estrogen intake (OR, 0.95; 95% CI, 0.82-1.10).32
Low-quality evidence showed that there may be an association between risk of bleeding and autoimmune disease (OR, 1.30; 95% CI, 0.77-2.19).8,32 However, we identified low-certainty evidence that there may be little to no association between risk of bleeding and malignancy (OR, 1.08; 95% CI, 0.42-2.77).8,32
Laboratory and physical examination factors
There is moderate-certainty evidence of a probable association between risk of bleeding and anemia as the reason for admission (OR, 5.15; 95% CI, 2.45-10.81),8,33 morbid obesity (BMI ≥40 kg/m2; OR, 3.08; 95% CI, 1.35-7.02),33 and low hemoglobin (<13 g/dL in men and <11.5 g/dL in women; OR, 2.33; 95% CI, 1.04-5.22).33
Discussion
Summary of findings
We evaluated prognostic factors for VTE and bleeding in hospitalized medical patients. We identified 23 prognostic factors for VTE and 15 for bleeding, some supported by moderate certainty of the evidence. Age, critical illness, CVC use, and autoimmune disease were prognostic of both outcomes. Obesity (BMI >30 kg/m2) and morbid obesity (BMI >40 kg/m2) were associated with VTE and bleeding, respectively. However, only age, critical illness, and autoimmune disease had the same quality of evidence for the 2 outcomes. This study is unique in many aspects including its comprehensiveness, the novelty of its findings, and its transparent approach.
Strengths
Methodologically, our study benefits from the rigorous methods, the breadth of our search, our duplicate and independent screening, the data abstraction process used, and our assessment of the certainty of evidence on the basis of a structured framework. Also, we conducted sensitivity analyses to compare different duration cutoffs for immobility and to address differences in type of outcome. Other strengths include the involvement of a number of content and methodological experts.
Limitations and challenges
A potential limitation in terms of the search strategy was the focus on prevention, which we applied to restrict the rather large number of citations that we identified in our searches and because we believed that we would not miss relevant studies. To confirm this, we checked a large random sample (n = 3000) of citations obtained from a search not including a restriction to the topic of prevention. We did not identify any study that would have fulfilled the inclusion criteria and, therefore, our original search was unlikely to have missed eligible studies. Also, time bias may be a potential limitation, as we identified some of the prognostic factors from older studies. This may overestimate VTE events when considering overall trends in the reduction of VTE events in hospitalized medical patients over time.
Potential limitations of the included studies relate to the inconsistency and variability across eligibility criteria in the original studies and variability in study design, study type, sample size, and definitions of the prognostic factors. Other challenges include inconsistency in methods of measurement used across studies and contamination of the population with nonmedical hospitalized patients.
Implications for practice
Our study identified candidate prognostic factors for VTE and bleeding that have been considered in the analysis of some developed and widely used RAMs in daily practice, such as the Caprini, IMPROVE (International Medical Prevention Registry on Venous Thromboembolism) VTE, IMPROVE bleed, and Padua models.7,40-42 However, some factors that we identified as having a probable association with VTE, based on our meta-analysis results, were not included or considered in the development of most of the RAMs, such as elevated CRP >10 mg/L (OR, 10.10), lower BI scores (BI ≤ 9; OR, 8.30), history of malignancy (OR, 3.20), and elevated heart rate (>100 beats/min; OR, 2.48). In addition, we found that an elevated fibrinogen level was inversely associated with DVT risk in patients with early stroke.35 This observation was opposite to the finding that elevated CRP, another acute-phase prognostic factor, showed an association with DVT risk. The authors speculated that this finding may be a result of fibrinogen depletion due to active clot formation.35 We believe that such reverse causation, given the study design, may be plausible. However, given the small sample size, the finding warrants further investigations in primary studies. In terms of bleeding, the candidate prognostic factor antithrombotic use showed mixed results in the different studies and was included only in 1 final model.32 However, we identified a probable association with the outcome when the individual results were subjected to meta-analysis,8,25,33 perhaps because of the limitation of the databases used that may not include all potential prognostic factors. Another reason that their findings may have been limited is the methods used in the development of RAMs for the multivariate analysis, such as automated procedures (eg, backward or forward) used for prognostic factor selection or selection of factors based on statistical significance at the univariate analysis stage. Therefore, the findings in our study ensure the consideration of all identified potential prognostic factors in the literature during the development of a RAM, a better assessment of the databases being used, and the comprehensiveness of the factors included in the databases. Studies in this systematic review included patients who received thromboprophylaxis, which may have altered the risk estimates. However, we controlled for the use of thromboprophylaxis in several ways. We selected studies only if they included a small fraction of patients receiving thromboprophylaxis (less than 10%) or if it was controlled for in the statistical analysis. Beyond that, given the general assumption that the relative risk related to a prognostic factor remains largely unaffected by administration of thromboprophylaxis (although the baseline risk of course might change), we used relative estimates of the risk. This assumption is supported by the observation that, in several studies, the relative estimates of risk were not influenced by adjustment for prophylaxis use in the statistical analyses. We believe that these measures should address the influence of thromboprophylaxis on the prognostic factor we addressed herein.
Implications for future research
Research may be needed to reevaluate existing RAMs, as the developers of the models may not have been able to use the variables we identified, given the limitations in the existing databases. However, a full development or improvement of a RAM that supports clinical practice requires further investigation of all the prognostic factors we identified in our study.
Conclusion
In this systematic review, we identified all reported relevant prognostic factors for VTE and bleeding in hospitalized medical patients. Some of these factors are not part of current risk prediction for VTE and bleeding in hospitalized medical patients. Our findings will help inform experts in developing population-based guidelines and accurate, user-friendly RAMs to better guide individual patient prophylactic management.
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
This work was supported by a subcontract (200-2016-92458) from the US Centers for Disease Control and Prevention (CDC), through Karna LLC.
The CDC, through Karna LLC, had no role in the detailed design and conduct of the study; the collection, management, analysis, and interpretation of the data; or the preparation of the manuscript. The findings and conclusions of this report are those of the authors and do not necessarily represent the official position of the CDC.
Authorship
Contribution: A.J.D. and H.J.S. were responsible for the conception and design of the study; A.J.D., S.G.K., R.C., I.E.-I., F.G., M.R., A.A., R.Z.M., and H.J.S. performed data acquisition; A.J.D., M.R., L.M., and H.J.S. performed data analyses; A.J.D., S.G.K., I.E.-I., M.C., M.K.G., L.M., F.A.S., A.C.S., M.B.S., S.W., N.A.Z., F.G., M.R., A.A., R.Z.M., A.I., E.A.A., and H.J.S. interpreted the results; A.J.D. and H.J.S. drafted the manuscript; and all authors critically revised the manuscript and approved the final version.
Conflict-of-interest disclosure: A.J.D., I.E.-I., A.I., E.A.A., and H.J.S. are members of the GRADE working group. A.C.S. has received remuneration for consulting from Bayer, Janssen, and Portola and research support grants from Boehringer Ingelheim, Janssen, and the Center for Medicare and Medicaid Services. A.C.S. also reported an intellectual conflict as the lead in the group that derived and validated the IMPROVE tool for VTE risk assessment in hospitalized medical patients. M.B.S. has received remuneration for consulting for Bayer, Janssen, Pfizer, and Portola and research support grants from Boehringer-Ingelheim, Janssen, Portola, and Roche. M.C. is a former board member (2013-2017) of the American Heart Association and chaired the committee that produced the American Society of Hematology (ASH) 2018 Guidelines for Management of Venous Thromboembolism: Prophylaxis for Hospitalized and Nonhospitalized Medical Patients (ASH 2018 Guidelines for Management of VTE). F.A.S. and N.A.Z. reported participating as panel members for the ASH 2018 Guidelines for Management of VTE. N.A.Z. also reported receiving honoraria in 2017 from ASH for the Highlights of ASH 2017 presentation (Dallas, New York, and Latin America). H.J.S. was cochair of the ASH 2018 Guidelines for Management of VTE committee and procured grant funding from the CDC for this study. The remaining authors declare no competing financial interests.
Correspondence: Holger J. Schünemann, Department of Health Research Methods, Evidence, and Impact, McMaster University, 1280 Main St West, Hamilton, ON L8N 3Z5, Canada; e-mail: schuneh@mcmaster.ca.