

PURPOSE: Diffuse large B-cell lymphoma (DLBCL) is a clinically heterogeneous disease. Patients exhibit a 30%-40% relapse/refractory rate on standard first-line therapy and are known to have poor outcomes with relapsed/refractory disease, indicating a significant need for novel therapies in high-risk groups. First-line clinical trials of novel therapies in DLBCL have consistently shown negative results in part due to improved outcomes in the control arm arising from eligibility criteria that limit enrollment of high-risk patient groups. We performed analyses to define evidence-based eligibility criteria to streamline enrollment of high-risk patient groups and select patient populations for first-line DLBCL trials.
METHODS: We enumerated eligibility criteria from 19 first-line DLBCL randomized controlled trials and defined Common (present in > 2/3 of analyzed studies), Moderately Common (present in 1/3-2/3 of studies), and Uncommon (present in < 1/3 of studies) criteria. Based on historical trends and clinical judgment, we proposed new eligibility criteria for DLBCL trials using 4 Common criteria (age at diagnosis, Eastern Cooperative Oncology Group performance status [ECOG PS], International Prognostic Index [IPI] score, and Ann Arbor stage). We assessed clinical trial eligibility among DLBCL patients in institutional, regional, and national data sets using these new eligibility criteria. Institutional datasets included: an Emory University DLBCL cohort [n = 329] and 3 DLBCL genomics studies (Reddy et al. [n = 761], Schmitz et al. [n = 361], and Chapuy et al. [n = 264]). Regional data included Surveillance, Epidemiology, and End Results (SEER) Program Georgia [n = 611] and SEER Iowa [n = 689] and national datasets included SEER national [n = 6,155] and SEER-Medicare [n = 11,066]. We calculated the sensitivity and specificity of combinations of proposed enrollment criteria and used receiver operating characteristic (ROC) plots to evaluate optimal combinations of criteria. Using the proposed criteria, we linked eligibility status with DLBCL genomics studies to determine patient-level mutational profiles and genetic clusters for the eligible population. We performed survival analysis according to eligibility status using the Kaplan-Meier method.
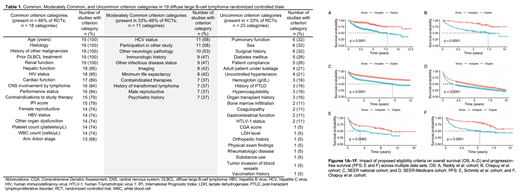
RESULTS: Across protocols for 19 first-line DLBCL trials spanning the R-CHOP era, we identified 52 eligibility criteria (18 Common, 11 Moderately Common, and 23 Uncommon; Table 1). Based on historical trends and clinical judgment, we proposed the following inclusion features using 4 Common criteria: age at diagnosis ≥ 18 years, ECOG PS 0-2, IPI score ≥ 2, and Ann Arbor stage II-IV. In comparing all possible combinations of proposed criteria, the combinations ECOG PS + stage (sensitivity 85%, specificity 51%), ECOG PS + IPI score (62%, 76%), and ECOG PS + IPI score + stage (59%, 77%) exhibited the greatest combined sensitivity and specificity across multiple data sets. MLL2 and MYD88 mutations were the most prevalent alterations among the eligible population in the Reddy et al. cohort, and 18q amplification and PIM1 mutation were the most prevalent alterations among the eligible Chapuy et al. cohort. Eligible patients had significantly inferior outcomes across multiple data sets (Figures 1A-1F).
CONCLUSION: We demonstrated the effective use of data-driven methods to identify parsimonious eligibility criteria for first-line DLBCL trials that identified eligible populations with worse outcomes across multiple datasets and uncovered relationships between eligibility criteria and ensuing cohort genomics. These techniques can be used to define potential trial populations and to project outcomes for novel agents in these populations. Next steps involve incorporating expert recommendations regarding essential and unnecessary enrollment criteria to improve trial design.
Flowers:AbbVie: Consultancy, Research Funding; BeiGene: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Denovo Biopharma: Consultancy; Gilead: Consultancy, Research Funding; Eastern Cooperative Oncology Group: Research Funding; National Cancer Institute: Research Funding; Burroughs Wellcome Fund: Research Funding; Karyopharm: Consultancy; AstraZeneca: Consultancy; Pharmacyclics/Janssen: Consultancy, Research Funding; Optimum Rx: Consultancy; Millenium/Takeda: Research Funding; Spectrum: Consultancy; Bayer: Consultancy; Acerta: Research Funding; Genentech, Inc./F. Hoffmann-La Roche Ltd: Consultancy, Research Funding; V Foundation: Research Funding; TG Therapeutics: Research Funding.

