

Background: Isovolemic hemodilution (IHD-RCE), an add-on to standard red cell exchange (RCE), was recently FDA-approved on select apheresis devices. Equipoise exists as to the degree of red cell unit reduction and time interval extension between procedures with IHD-RCE. Also, concern has been raised that the transient hematocrit (Hct) decrease and potential hypotension with IHD-RCE causes ischemic brain injury, especially with Moya Moya disease. Again, there is equipoise, with only one of 4 studies reporting increased hypotension and no studies of ischemic brain injury with IHD-RCE. We therefore conducted a retrospective crossover study of efficacy and safety of IHD-RCE in our sickle cell disease patients, three of whom had Moya Moya, and report follow-up brain MRI/MRA data, heretofore not reported in the literature.
Study design: This was a retrospective review of patients who crossed over from standard RCE (Cobe Spectra) to IHD-RCE (Spectra Optia). The IHD phase used normal saline for replacement fluid. Minimum (post-IHD) hematocrits (Hcts) and post-procedure Hcts were based upon pre-procedure Hcts as per Matevosyan et al, JCA 2012. Pre-procedure CBCs, reticulocyte counts, and serum ferritins were drawn within 72 hours of the procedure and post-procedure CBCs drawn immediately post-procedure. All red cell units were leuko-reduced, CEK matched, and less than 15 days old when possible.
Methods: The same number of procedures were analyzed for standard RCE and IHD-RCE, with the RCE procedures most recent to crossover to IHD-RCE used for comparison. Means of continuous variables were calculated for each patient; means and standard deviations of the patient means are shown, unless otherwise indicated. Paired t-testing was used to compare IHD-RCE to RCE († in tables indicates p-value < 0.05)
Results:
Patients: All 6 patients (3 M, 3 F) were black; 5 had HbSS and 1 had SB+thal. The indication for RCE was stroke prophylaxis in four, 3 of whom had Moya-Moya disease, and frequent vaso-occlusive crisis (VOC) in two. Mean patient age at the time of first IHD-RCE was 15 ± 2 years, and a mean 26 ± 12 procedures of each procedure type was analyzed for IHD-RCE to RCE comparisons. Patient total blood volume (TBV) significantly increased from the RCE to IHD-RCE periods and was accounted for in the analysis.
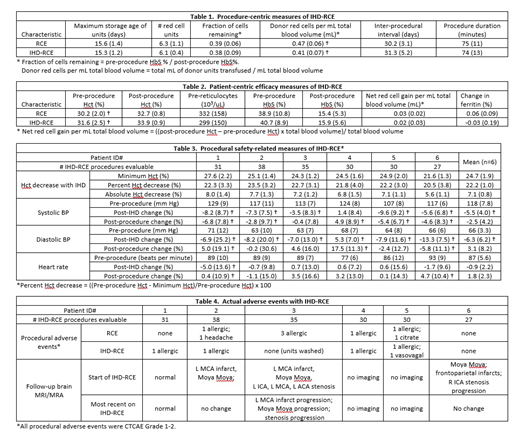
Procedure-centric measures (Table 1). Despite increasing TBV, red cell unit usage did not increase, and the volume of donor red cells transfused per mL TBV significantly decreased with IHD-RCE. There was no increase in inter-procedural interval.
Patient-centric efficacy measures (Table 2): Despite the decreased volume of donor red cells transfused per mL TBV, and similar post- and pre-procedure HbS %s between IHD-RCE and RCE, the pre-procedure Hct was slightly (5%) increased with IHD-RCE.
Procedural safety-related measures (Table 3): Although there were statistically significant drops in systolic and diastolic blood pressures (BP) post-IHD compared to pre-procedure BP, the degrees (about -6%) were mild. By procedure end, there were no overall significant differences in BP from pre-procedure BP. In addition, there was no overall significant change in heart rate post-IHD or post-procedure.
Actual patient adverse events (Table 4): One patient had a single possibly IHD-related Grade 2 symptomatic (dizziness) vasovagal event, occurring at procedure end and resolved with normal saline bolus. All 4 patients on IHD-RCE for stroke prophylaxis had follow-up MRI/MRA after switching to IHD-RCE. One patient showed new silent strokes and vasculopathy but her prior MRI/MRA predated her standard RCE period. One patient who had progressed on standard RCE had no progression on IHD-RCE. The other two patients had stable MRI/MRA.
Conclusion: When reducing pre-procedure Hct by 20-24% during the IHD phase, our data confirm the 11-13% reduction in red cell unit usage with IHD-RCE reported by Sarode et al, JCA 2011 and Hequet et al, Transfusion 2019, but do not support an increased inter-procedural interval of 16 days as per Sarode et al. Most patients had a mild (< 15%) and asymptomatic drop in systolic and diastolic BPs with IHD-RCE; a minority also had a very mild (<5%) HR increase; use of 5% albumin rather than saline replacement may mitigate these drops. MRI/MRA follow-up did not show any definitive ischemic brain injury associated with IHD-RCE.
No relevant conflicts of interest to declare.

