

TO THE EDITOR:
In the United States, Blacks and Hispanics are less likely than Whites to survive acute leukemias and other serious hematologic malignancies.1-3 Allogeneic hematopoietic cell transplantation (HCT) plays an important role in the treatment of high-risk hematologic malignancies, and 1 factor likely contributing to this disparity is the limited availability of 8/8 HLA-matched unrelated donors for persons of color (POC).4 Although most POC have access to 7/8 matched unrelated donors, mismatching is associated with increased risk for acute graft-versus-host disease (aGVHD), transplant-related mortality (TRM), and diminished overall survival (OS).5
The multicenter phase 2 trial Abatacept 2 (ABA2, NCT01743131), compared standard GVHD prophylaxis with a calcineurin inhibitor and short-course methotrexate (CNI/MTX) to CNI/MTX plus the costimulation blockade agent, cytotoxic T-cell lymphocyte-4-immunoglobulin (abatacept) in unrelated donor transplantation. Patients with HLA-matched donors (8/8; match unrelated donor [MUD]) were assigned to a randomized, placebo-controlled stratum, whereas patients with mismatched donors (7/8, MMUD) were assigned to a single-arm, open-label stratum (compared with a prespecified Center for International Blood and Marrow Transplant Research registry cohort). ABA2 demonstrated reductions in aGVHD with abatacept in both MUD and MMUD HCT, but its effects were especially large in MMUD, where it was associated with a marked decrease in severe aGVHD and TRM as well as improved severe aGVHD-free survival (SGFS), relapse-free survival (RFS), and OS.6 Based on these observations, we hypothesized that abatacept could abrogate the risks associated with HLA mismatching. To rigorously assess this, we performed a post hoc analysis of trial data, comparing outcomes in patients with MMUD receiving CNI/MTX and abatacept to patients with MUD receiving CNI/MTX alone.
Patients ≥6 years of age with a hematologic malignancy undergoing unrelated donor HCT were enrolled to the trial between 2013 and 2017. For conditioning, participants received 1 of 3 myeloablative regimens (busulfan/fludarabine, busulfan/cyclophosphamide, or total body irradiation/cyclophosphamide) or reduced toxicity fludarabine and melphalan. All patients received T cell-replete grafts, and the use of lymphocyte depleting antibodies/serotherapy was prohibited. For GVHD prophylaxis, patients received either cyclosporine or tacrolimus through at least day +100 and IV methotrexate (15 mg/m2 on day +1 and 10 mg/m2 on days +3, +6, and +11). MUD HCT recipients were randomized (1:1) to receive abatacept or placebo, and all MMUD HCT recipients received abatacept, which was delivered as 4 (10 mg/kg) IV doses on days −1, +5, +14, and +28. The institutional review boards of Emory University, Fred Hutchinson Cancer Research Center, and the Dana-Farber Cancer Institute approved the study, which was conducted in accordance with the Declaration of Helsinki.
In this post hoc comparison of MMUD HCT with CNI/MTX/abatacept (MMUD/aba) to MUD HCT with CNI/MTX/placebo (MUD/placebo), the primary endpoint was the cumulative incidence of severe (grade 3-4) aGVHD at day +100. Secondary endpoints included SGFS, RFS, GVHD-free (absence of severe acute or moderate-to-severe chronic GVHD)/Relapse Free-Survival (GRFS), and OS. Multivariate models were constructed for all clinical endpoints. Analysis was conducted using SAS v. 9.4 (SAS Institute, Cary, NC, USA) or R (r-project.org, Vienna, Austria).
Forty-three patients received MMUD/aba; 69 received MUD/placebo. A total of 82.1% of the entire group had acute myeloid leukemia, acute lymphoblastic leukemia, or myelodysplastic syndrome; 73.2% received myeloablative conditioning and 58.0% received peripheral blood stem cell transplantation. The median age was 40.0 years (range, 6.6-76.6). Recipient age, performance status, disease, disease stage, conditioning intensity (myeloablative vs reduced intensity) were similar across the 2 groups. The groups differed only by distribution across conditioning regimens (P = .035): a greater proportion (18.6% vs 2.9%) of MMUD/aba patients received busulfan and fludarabine and a smaller proportion of MMUD/aba patients received totally body irradiation and cyclophosphamide (25.6% vs 37.7%). There were 30.2% non-White MMUD/aba patients vs 11.6% non-White MUD/placebo patients (P = .087; supplemental Table 1).
There were no differences in neutrophil or platelet engraftment. The cumulative incidence of grade 3-4 aGVHD by day 100 was 2.3% (95% confidence interval [CI], 0.2-10.7) in the MMUD/aba group and 14.8% (95% CI, 7.5-24.3) in the MUD/placebo group (P = .03; Figure 1). The cumulative incidence of moderate to severe chronic GVHD by 1 year was 57.9% (95% CI, 40.7-71.8) and 41.3% (95% CI, 27.7-54.4) in the MMUD/aba and the MUD/placebo groups, respectively (P = .12). There were no significant differences in the day 180 cumulative incidence of cytomegalovirus or Epstein-Barr virus viremia (defined as any detectable copy number) between the 2 groups (cytomegalovirus 37.2%, 95% CI, 24.7% to 53.4% versus 50.5%, 95% CI, 38.8% to 63.4%, P = .20, and Epstein-Barr virus 46.5%, 95% CI, 33.0-62.4 vs 33.3%, 95% CI, 22.5-47.5, P = .14 in the MMUD/aba and MUD/placebo groups, respectively). With a median follow-up of 25 months in survivors, the 2-year cumulative incidence of TRM was 16.7% (MMUD/aba, 95% CI, 6.4-31.3) and 16.1% (MUD/placebo, 95% CI, 8.5-25.9; P = .78); the cumulative incidence of relapse was 9.3% (MMUD/aba, 95% CI, 2.9-20.3) and 23.6% (MUD/placebo, 95% CI, 14.2-34.3; P = .07); RFS was 74.0% (95% CI, 56.3-85.4) and 60.3% (95% CI, 47.6-70.9; P = .08) for the MMUD/aba and MUD/placebo groups, respectively (Figure 1). SGFS through day 180 was 97.7% (95% CI, 84.6-99.7) in the MMUD/aba group and 82.0% (95% CI, 70.5-89.4) in the MUD/placebo group (P = .015). GRFS through 1 year was 34.9% (MMUD/aba, 95% CI, 21.2-48.9) and 34.7% (MUD/placebo, 95% CI, 23.6-46.1; P = .58). Two-year OS was 73.6% (95% CI, 54.5-85.7) and 64.0% (95% CI, 51.2-74.3; P = .20), respectively. Controlling for age, performance score, disease stage, graft type, and conditioning regimen did not impact any of the comparisons (Figure 2). The adjusted hazard ratios (MUD/placebo group as baseline <1.0 favorable) for RFS and OS in the MMUD/aba patients were 0.60 (95% CI, 0.28-1.28; P = .19) and 0.77 (95% CI, 0.34-1.71; P = .51), respectively. There were no differences in absolute lymphocyte count, CD4+, and CD8+ T cells between the 2 groups at day 100 or 1 year (data not shown). Although outside the scope of the present analysis, outcomes of MMUD/aba patients were also similar to those of the 8/8 MUD patients randomly assigned to receive abatacept (MUD/aba) on the ABA2 trial rather than placebo.6
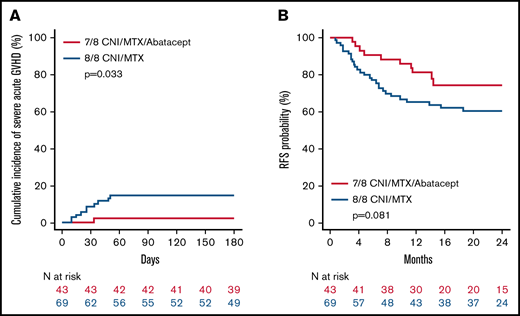
Cumulative incidence of severe (grade 3-4) aGVHD and RFS comparing 7/8 CNI/MTX/abatacept to 8/8 CNI/MTX/placebo. (A) Cumulative incidence of 6-month severe aGVHD by treatment group. 7/8 MMUD with CNI/MTX/abatacept 2.3% (95% CI, 0.2-10.7); 8/8 MUD with CNI/MTX/placebo 14.8% (95% CI, 7.5-24.3). (B) Cumulative incidence of 2-year RFS: 7/8 MMUD with CNI/MTX/abatacept 74.0% (95% CI, 56.3-85.4); 8/8 MUD with CNI/MTX/placebo 60.3% (95% CI, 47.6-70.9). In each panel, red = 7/8 MMUD with CNI/MTX/abatacept; blue = 8/8 MUD with CNI/MTX/placebo.
Cumulative incidence of severe (grade 3-4) aGVHD and RFS comparing 7/8 CNI/MTX/abatacept to 8/8 CNI/MTX/placebo. (A) Cumulative incidence of 6-month severe aGVHD by treatment group. 7/8 MMUD with CNI/MTX/abatacept 2.3% (95% CI, 0.2-10.7); 8/8 MUD with CNI/MTX/placebo 14.8% (95% CI, 7.5-24.3). (B) Cumulative incidence of 2-year RFS: 7/8 MMUD with CNI/MTX/abatacept 74.0% (95% CI, 56.3-85.4); 8/8 MUD with CNI/MTX/placebo 60.3% (95% CI, 47.6-70.9). In each panel, red = 7/8 MMUD with CNI/MTX/abatacept; blue = 8/8 MUD with CNI/MTX/placebo.
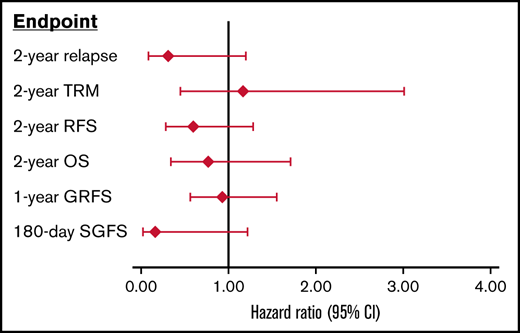
Multivariate analysis of transplant outcomes comparing 7/8 CNI/MTX/abatacept to 8/8 CNI/MTX/placebo. Forest plot depicting the results of multivariate analysis with adjusted hazard ratio (HR; diamonds, with 95% CIs shown with bars) comparing 7/8 MMUD with CNI/MTX/abatacept to 8/8 MUD with CNI/MTX/placebo. In this Forest plot, the adjusted HR uses 8/8 CNI/MTX/placebo as baseline, with HR <1.0 being favorable for the 7/8 CNI/MTX/abatacept group. This multivariate analysis controlled for age, performance score, disease stage, graft type, and conditioning regimen. Shown are adjusted HR for relapse, TRM, RFS, OS, GVHD-free-relapse-free survival (using the modified GFRS definition, with severe aGVHD, moderate-to-severe chronic GVHD, relapse, and death considered as events), and SGFS.
Multivariate analysis of transplant outcomes comparing 7/8 CNI/MTX/abatacept to 8/8 CNI/MTX/placebo. Forest plot depicting the results of multivariate analysis with adjusted hazard ratio (HR; diamonds, with 95% CIs shown with bars) comparing 7/8 MMUD with CNI/MTX/abatacept to 8/8 MUD with CNI/MTX/placebo. In this Forest plot, the adjusted HR uses 8/8 CNI/MTX/placebo as baseline, with HR <1.0 being favorable for the 7/8 CNI/MTX/abatacept group. This multivariate analysis controlled for age, performance score, disease stage, graft type, and conditioning regimen. Shown are adjusted HR for relapse, TRM, RFS, OS, GVHD-free-relapse-free survival (using the modified GFRS definition, with severe aGVHD, moderate-to-severe chronic GVHD, relapse, and death considered as events), and SGFS.
Taken together, these results suggest the addition of abatacept to standard CNI/MTX mitigates the disadvantages of mismatching by greatly reducing the risks of severe aGVHD and NRM without increasing the risk of relapse. Recognizing the limitation of a post hoc analysis with a relatively small sample size, the strengths of this study include analyses derived from a single prospective, multicenter trial, and the use of multivariate analysis to adjust for the effects of potential confounders (Figure 2). As previously reported and based on findings herein, the 4-dose schedule of abatacept did not reduce the risk for chronic GVHD.6 To address this, a multicenter, randomized controlled trial (ABA3, NCT04380740) will be conducted to determine whether an 8-dose regimen of abatacept (last dose at day +150) can better prevent chronic GVHD, and, thereby, improve severe (grade 3-4) aGVHD-free, moderate-to-severe chronic GVHD-free, relapse-free survival.
The results of recent clinical trials and registry studies suggest that other approaches, including posttransplant cyclophosphamide (PT-Cy), also hold promise for patients receiving MMUD transplants for hematologic malignancies,7-9 with PT-Cy effective at preventing both acute and chronic GVHD in MMUD.8,9 Of interest, patients in the myeloablative conditioning stratum of the recent National Marrow Donor Program-sponsored PT-Cy trial had 1-year GRFS similar to that of MMUD/aba patients (38% in the National Marrow Donor Program PT-Cy patients vs 34.9% in MMUD/aba patients). However, the PT-Cy patients had inferior 6-month SGFS (68% for MMUD/PT-Cy vs 97.7% for MMUD/aba).9 Together, POC account for a large proportion of enrollment in both the ABA2 and PT-Cy trials. These studies document the emergence of multiple strategies that could make MMUD HCT an effective alternative for HCT, and, thereby, lessen disparities in outcomes affecting POC with hematologic malignancies.
As experience grows with MMUD HCT, especially after myeloablative conditioning as in the ABA2 trial, it will be important to compare the differing approaches to GVHD prophylaxis in these patients, as well as directly comparing MMUD HCT and haploidentical HCT. These studies should be large enough to explore the comparative effects across subgroups. Such studies may prove that a 1-size-fits-all approach is suboptimal and that certain conditions (for example, the availability of a young donor10,11 ) may favor 1 approach over the other for a given patient.
Acknowledgments: The authors gratefully acknowledge the patients who participated in this study and their families. We thank the clinical research staff and caregivers at all participating sites.
This study was funded by grants from the National Institutes of Health National Heart, Lung, and Blood Institute (2R01 HL095791), National Institutes of Health/Food and Drug Administration (R01 FD004099), and CURE Childhood (https://curechildhoodcancer.org) to L.S.K.
Contribution: M.Q., B.W., A.L., J.T.H., and L.S.K. developed the trial; M.Q., B.W., A.L., L.S.K., and J.T.H. designed the secondary analysis; S.G. performed the statistical analyses; S.W.C., J.D., C.D., R.G., M.G., A.C.H., D.J., N.L., M.N., N.F., M.A.P., A.P., K.R.S., G.A.Y., and E.K.W. were local investigators; M.Q., B.W., A.L., L.S.K., and J.T.H. wrote the manuscript; and all authors have contributed to and approved the final manuscript.
Conflict-of-interest disclosure: M.Q. reports grants and personal fees from Bristol Myers Squibb during the conduct of the study, and consulting fees from Medexus, Jazz Pharmaceuticals, and Mesoblast; in addition, she has a patent “Method to prevent relapse after transplant” that is pending. B.W. reports personal fees from Bristol Myers Squibb during the conduct of the study andhe has a patent “Method to prevent relapse after transplant” that is pending. A.L. reports grants and personal fees from Bristol Myers Squibb during the conduct of the study and a patent “Method to prevent relapse after transplant” that is pending. J.T.H. reports grants and personal fees from Bristol Myers Squibb during the conduct of the study and a patent “Method to prevent relapse after transplant” that is pending. L.S.K. is on the scientific advisory board for HiFiBio; reports research funding from Kymab Limited, Magenta Therapeutics, BlueBird Bio, and Regeneron Pharmaceuticals; reports consulting fees from Equillium, FortySeven Inc, Novartis Inc, EMD Serono, Gillead Sciences, and Takeda Pharmaceuticals; and reports grants and personal fees from Bristol Myers Squibb during the conduct of the study and grants and personal fees from Bristol Myers Squibb outside the submitted work; her conflict-of-interest with Bristol Myers Squibb is managed under an agreement with Harvard Medical School; in addition, she has a patent “Method to prevent relapse after transplant” that is pending and a patent “Method to prevent GVHD after transplant” with royalties paid. S.S. reports grants and personal fees from Bristol Myers Squibb outside the submitted work. The remaining authors declare no competing financial interests.
Correspondence: John T. Horan, Stem Cell Transplantation Program Dana-Farber/Boston Children’s Cancer and Blood Disorders Center, 450 Brookline Ave, Boston, MA 02115; e-mail: john_horan@dfci.harvard.edu.

