

Abstract
Exercise is increasingly recognized as important to cancer care. The biology of how exercise improves outcomes is not well understood, however. Studies show that exercise favorably influences the immune system in healthy individuals (neutrophils, monocytes, natural killer cells, T cells, and a number of cytokines). Thus, exercise in patients with hematologic cancer could significantly improve immune function and tumor microenvironment. We performed a literature search and identified 7 studies examining exercise and the immune environment in hematologic malignancies. This review focuses on the role of exercise and physical activity on the immune system in hematologic malignancies and healthy adults.
Background
Hematologic malignancies include a broad group of hematopoietic and lymphoid neoplasms. For instance, it is estimated that there are 13.8 new cases of leukemia,1 19.4 new cases of non-Hodgkin lymphoma (NHL),2 2.5 new cases of Hodgkin lymphoma,3 and 6.7 new cases of myeloma4 per 100 000 people per year. Although increasing knowledge of cytogenetics and molecular properties greatly adds to prognostication within a particular disease group, considerable variability exists, and these markers are generally not modifiable.5
Understanding modifiable lifestyle factors, including diet and levels of physical activity, is an important component to improving outcomes in hematologic malignancies. Currently, some hematologic malignancy patients may receive physical therapy during and after treatment; however, this therapy often occurs when a limitation is noted.6 Exercise, conversely, tends to be more broad in that it also occurs to maintain or improve overall physical fitness.6,7 In fact, it is recommended that all adults, including older adults, get a minimum of 150 minutes of moderate-intensity exercise per week.8 Thus, incorporating exercise is an intervenable aspect of care that is relevant to all patients with hematologic malignancies. Physical activity and structured exercise are of particular biological interest given their impact on the immune system in healthy individuals.9,10 Specifically, exercise can improve cellular functions, including microbial phagocytosis, T-cell proliferation, vaccine responses, and tumor cell killing.
Defining these effects in hematologic malignancies is especially relevant, as immune dysfunction is associated with significant morbidity and mortality. In addition, increasing therapeutic options are directed at the immune system but clinical success is variable, potentially from failure to fully restored immune function.11,12 Ultimately, exercise could serve as an important adjunct to cancer care. Exercise in adult bone marrow transplant patients has been previously studied13-15 ; however, as this is evaluating a new and developing immune system in a presumably disease-free state, this topic was outside the scope of this review. The current review focused on: (1) the immunomodulatory effects of exercise in relation to hematologic malignancies; and (2) the data regarding the impact of exercise on the immune environment in hematologic malignancies.
Exercise and clinical outcomes in hematologic malignancies
Several exercise studies and reviews of various clinical outcomes, including quality of life (QoL), symptom burden, and survival, exist. Most notably, the 2019 Cochrane Review by Knips et al16 evaluated 18, mostly small, randomized controlled trials (RCTs) for efficacy, safety, and feasibility of aerobic physical exercise in adults with hematologic malignancies. The primary end point of survival was assessed in only 1 RCT, and unlike solid tumor survival, evidence was inconclusive.17-21 Although exercise may improve fatigue and depression, evidence was inconclusive regarding QoL and physical functioning. These findings do not reflect the potential absence of patient benefit from exercise; rather it shows the lack of RCTs and broad variability in design/measured outcomes that make generalizability and comparison between aerobic exercise trials difficult. The main conclusion by the authors was the need for larger trials with longer follow-ups.16 That being said, several smaller disease-specific studies (eg, lymphoma and multiple myeloma) suggest positive trends with increasing physical activity and QoL.22-24
In a study of patients with lymphoma actively undergoing chemotherapy, Streckmann et al25 conducted an RCT assessing 36 weeks of supervised exercise training consisting of twice weekly balance, endurance, and strength exercises. Compared with the control group, the exercise training group had significant improvements in therapy-related toxicities, physical function, and QoL (European Organization for Research and Treatment of Cancer Quality of Life Questionnaire–Core 30). Similarly, aerobic, strength, and balance training were found to be safe and feasible with a trend toward improved QoL (European Organization for Research and Treatment of Cancer Quality of Life Questionnaire–Core 30) in patients with acute myeloid leukemia (AML) undergoing inpatient chemotherapy induction.26 Furthermore, as little as 7 weeks of interval-based treadmill walking was sufficient to negate the historically observed treatment-related loss of physical function during chemotherapy for 6 different hematologic cancers.27 In the Healthy Exercise for Lymphoma Patients trial, 12 weeks of supervised aerobic exercise improved overall QoL (Functional Assessment of Cancer Therapy–Anemia Scale), physical function, depression, and fatigue compared with usual care.28 As such, these studies highlight the potential benefits of exercise during active treatment of various hematologic malignancies.
Participation in a structured exercise program during active treatment may not be feasible for all patients. Exercise after therapy has been explored to regain fitness and improve cancer outcomes. As assessed in 37 patients after chemotherapy completion, a 12-week aerobic and resistance exercise program was associated with significant cardiometabolic, strength, fatigue, and QoL improvements (Functional Assessment of Cancer Therapy–General questionnaire) compared with usual care.29 In a cross-sectional analysis, Husson et al30 assessed fatigue and physical activity through longitudinal surveys of patients with lymphoma over a 2-year period. Although the results were somewhat complicated by the fact that study patients included active treatment, posttreatment, and treatment naive patients, higher levels of physical activity (meeting European Physical Activity Guidelines) was associated with significantly less fatigue according to the Fatigue Assessment Scale.
Together, these studies highlight the potential benefits of exercise and physical activity in the management of patients with hematologic cancer, positively influencing outcomes such as QoL and symptom management in a number of studies. This finding is particularly imperative as better QoL is increasingly recognized as being associated with reduced mortality and improved overall survival.31-34
Immunomodulatory effects of physical activity and structured exercise
Although recognizing the impact of physical activity on clinical outcomes in hematologic malignancies is essential, understanding the biology of physical activity in these cancers also is crucial. One potential mechanism is through immunomodulation. The following section discusses the important cellular components of the immune system, their role in hematologic malignancies, and the existing evidence supporting how exercise can potentially modify those cells to improve cancer outcomes (Figure 1). The section concludes with a discussion of the hematologic studies that have assessed immune responses after exercise exposure.
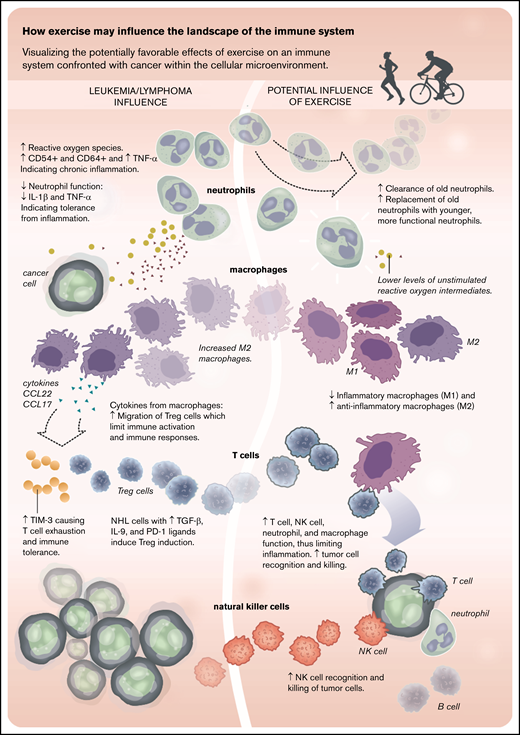
Diagram of how exercise may influence the landscape of the immune system. ↑, increased; ↓, decreased; PD-1, programmed cell death protein 1; TGF-β, transforming growth factor-β; TNF, tumor necrosis factor.
Diagram of how exercise may influence the landscape of the immune system. ↑, increased; ↓, decreased; PD-1, programmed cell death protein 1; TGF-β, transforming growth factor-β; TNF, tumor necrosis factor.
T cells
Enhancing T-cell function has become an effective therapeutic approach in solid and hematologic malignancies. This includes checkpoint inhibitors,35 genetically modified chimeric antigen receptor T cells,36 bispecific antibodies linking the malignant cell to the target,37 and adoptive T-cell therapy.38 In hematologic malignancies, underlying T-cell dysfunction is common, which can be worsened by traditional chemotherapeutic treatments, leading to severe T-cell depletion. Improving T-cell function holds significant promise, but limitations include significant toxicities, variable response rates, and large economic burden for both the patient and the health care system.39,40 Thus, alternative adjunctive therapy to improve T-cell function is needed.
The field of exercise immunology mainly concentrates on T cells of healthy adults and has been extensively reviewed.41-46 Most T-cell exercise studies focus on T-cell phenotype changes rather than functional changes. However, several recent studies have focused on exercise and the impact on T-cell immune-aging, termed immunosenescence. Immunosenescence is associated with an increased mortality risk.47-49 Exercise exposure can improve features of immunosenescence, such as reduced dysfunctional senescent T cells (KLRG1pos/CD57pos/CD28neg),50 improved thymic output,51 and improved vaccine responses.52 In a study comparing older adults (aged 55-79 years) who were either sedentary or “master athletes” (men with the ability to cycle 100 km in 6.5 hours or women with the ability to cycle 60 km in 5.5 hours), immunosenescence was reduced.51 Specifically, master athletes had higher numbers of naive CD4+ T-cell and recent T-cell thymic emigrants, suggestive of improved thymic and T-cell functions. Furthermore, immune composition of T cells for master athletes was similar to those of young (aged 20-36 years) healthy adults.
A single session of cycling at 10% to 15% above lactate threshold was sufficient to improve ex vivo generation of adenovirus-specific T cells.53 Similarly, a single session of exercise in a young healthy cohort showed increased cytotoxic activity of T cells toward the tumor antigens MAGE and PRAME.54 Specifically, rapid ascent of 10 flights of stairs resulted in a 3-to 6-fold increase in cytotoxic lymphocytes specific for MAGE-A4 and PRAME, tumor-associated antigens found in many hematologic malignancies. This finding suggests that both chronic exercise training and single exercise sessions potentially could improve clinically relevant T-cell functions and offer another avenue for T-cell adoptive therapy.
Natural killer cells
Defects in natural killer (NK) cell cytotoxicity are prevalent in hematologic malignancies and those at higher risk of cancer such as the elderly. Activation and modulation of NK cells have been shown to be effective immunotherapy in many cancer settings.55-58 NK cells are innate immune-effector lymphocytes that recognize and kill malignant cells and promote enhanced T-cell responses through cytokine and chemokine production augmenting NK-cell-to-tumor-cell direct cytotoxicity (NKCA). Transformed malignant cells, unlike healthy cells, often express ligands such as the major histocompatibility complex class 1 chain-related proteins A and B (MICA and MICB).59 MICA and MICB are ligands for the natural cytotoxicity receptor NKG2D, leading to tumor cell destruction.60 Conversely, cytotoxicity is downregulated by engagement of human leukocyte antigen (HLA)–specific inhibitory receptors such as killer immunoglobulin-like receptors, protecting normal host tissue. Expression of normal HLA class I molecules on tumor cells and soluble MICA downregulate NK cell cytotoxicity.61,62 Increased expression of tumor cell HLA class I is associated with impaired NK cytotoxicity in multiple hematologic malignancies. Decreased NKG2D expression on NK cells in patients with AML, chronic lymphocytic leukemia (CLL), and multiple myeloma is associated with increased levels of tumor-derived soluble MICA and MICB, leading to NK cell anergy.
Several hematologic malignancy drugs exhibit influence on NK cell cytotoxicity. The immunomodulatory drugs lenalidomide and pomalidomide induce NK cell proliferation and enhance NK-mediated cytotoxicity.63 Proteasome inhibitors (eg, bortezomib) used to treat multiple myeloma, especially in combination with radiation or inhibition of glycogen synthase kinase, increase NKG2D expression while downregulating HLA molecules on tumor cells.64,65
NK cells are highly responsive to acute and chronic exercise training in healthy individuals and cancer survivors. During each single session of aerobic exercise, there is an increased number and altered composition of NK cells in the blood, which return to pre-exercise levels shortly after exercise cessation.66-69 Mobilization occurs from tissues into the blood during exercise, before an egress from the blood back to tissues upon cessation of exercise. This action explains the early exercise-related NK cell work which saw the NKCA increase because the tumor-cell-to-NK-cell ratio was reduced.70-73 When these ratios are adjusted for the exercise-mediated increase in NK cell absolute numbers, there is no increase in HLA-negative NKCA on a per NK cell basis in healthy individuals against lymphoma and myeloma tumor cell lines.67,74 Bigley et al67 suggest that during the egress after exercise, the cells that are left in the blood of healthy adults have an increased NKCA against these HLA-expressing cell lines but not HLA-negative cells. These cytotoxic properties are associated with alterations for inhibitory (eg, CD158b) and activatory (eg, NKG2C) receptors, resulting in the potential of exercise to increase tumor cell killing during and after exercise.
Cross-sectional studies suggest positive associations between increased longitudinal aerobic fitness or exercise exposure and NKCA.9,10,75,76 However, likely due to methodologic differences, other studies suggest no changes.70,77,78 In a preclinical model, Pedersen et al79 showed that after as few as 30 days of free-wheel running, mice with 1 of 5 solid tumors exhibited up to 60% reduction in tumor burden, mediated by NK cell redistribution.
Altogether, NK cells are critical for the control of tumor cells. Exercise can improve NK cell effector functions and their antitumor properties. Exercise likely reconstitutes functional NK cells and exposes malignant cells to “newer” NK cells that are unaffected by tumor-associated suppression.
Neutrophils
Neutrophil functions in most patients with hematologic malignancies are impaired, partly due to bone marrow suppression from treatment or the malignancy itself, leading to increased infections and complications. Neutrophils mediate host defense by phagocytosis and intracellular killing of pathogens, release of antimicrobial peptides, release of immunomodulatory cytokines and chemokines, and formation of histone-bound DNA traps, known as neutrophil extracellular traps.80 In older adults, primary functions of neutrophils are reduced or impaired, leading to an increased risk of infections and poor resolution of tissue insults.81
There is a growing body of evidence regarding the role of exercise on neutrophil functions. Recently, in older adults with rheumatoid arthritis, 10 weeks of interval style walking was associated with improved neutrophil phagocytic and chemotactic capacity toward bacterial insults.82 Older healthy adults (aged >60 years) who engage in at least 10 000 steps per day had better neutrophil pathogen-related chemotactic capacity than age-matched adults who walk only 5000 steps per day.83 In younger healthy adults, chemotaxis, phagocytosis, formation of neutrophil extracellular traps, and mitochondrial functions have been improved by either an acute session or weeks of exercise training.84-87 Neutrophil dysfunction is associated with poor outcomes in both solid and hematologic malignancies. If exercise can be used as an adjuvant to improve neutrophil functions, along with the improvements in T-cell and NK cell function discussed earlier, this may improve cancer outcomes.
Monocytes/macrophages
A growing body of literature addresses the role that monocytes and macrophages play in the progression of hematologic malignancies. Higher circulating absolute monocyte counts (AMCs) at diagnosis are associated with worse outcomes. In CLL, the diagnostic AMC value is also associated with worse overall survival.88,89 Furthermore, the ratio of absolute lymphocyte counts (ALCs) to AMCs is associated with a more indolent form of the disease.90 It has been suggested that blood monocytes and tissue macrophages promote the survival, proliferation, and resistance to drugs of malignant cells. Therefore, monocytes can be considered an alternative target to treatment of hematologic malignancies. Exercise training may be a viable option to alter the monocyte/macrophage fate and influence on circulating malignant cells.
Increased physical fitness is associated with less CD16pos nonclassical and intermediate monocytes.82,84,91,92 These monocytes, compared with CD16neg monocytes, are considered to have increased proinflammatory cytokine secretion and are a likely cellular candidate promoting enhanced survival of malignant cells.93-95 Timmerman et al91 suggested that inactive older adults had more CD16pos monocytes than matched active adults. In addition, 10 weeks of interval exercise training was sufficient to reduce the amount of CD16pos monocytes in healthy adults and older adults with rheumatoid arthritis.82,84 Other monocyte markers of exercise-mediated improved function include increased CD80 expression, a critical costimulatory molecule in vaccine responses, and increased phagocytosis of bacteria.84,96
Moreover, there is a delicate balance between the macrophage subtypes generated from monocytes: M1 (inflammatory macrophages) and M2 (anti-inflammatory macrophages). Increased M1 can lead to complications from chronic inflammation in adults, whereas tumor survival is often promoted by an accumulation of M2. Exercise training switched the composition of M1s to more M2s in adipose tissue of mice.97 Exercise training in cancer patients likely induces a beneficial switch to increased M2s in adipose and muscle tissue, as evidenced by the muscle adaptation and reduced body fat percentage. However, in the tumor microenvironment, this is unknown, and more research is required.
B cells
There is considerably less research regarding B cells in relation to exercise. These cells follow a typical acute exercise pattern in which numbers increase before decreasing below basal levels during recovery from exercise.42,98 Specifically, acute exercise in young adults mobilizes immature (CD27neg/IgDneg/CD10pos) B cells to the greatest extent. Total B-cell numbers increased after exercise, including memory (CD27pos/CD38neg) and naive (CD27neg/CD10neg) cells. Although investigational, it is possible that acute exercise serves as a method to invigorate B cells.41 Because B-cell immunoglobulin production is critical to vaccine responses, studies showing benefits of exercise on vaccine responses can be interpreted as improving B-cell functions.99 Furthermore, compared with inactive older adults, master athletes exhibited signs of increased frequencies of B-regulatory cells, a potentially important cell in the regulation of immune responses.51
In summary, a number of dysfunctional cells either directly involved in the hematologic malignancies or in the microenvironment of these cancers are affected by exercise in healthy individuals and thus could have the potential to be influential in hematologic malignancies.
Exercise intervention and immune responses in hematologic malignancies
Few studies have assessed exercise and immune function in hematologic malignancies. We discuss these findings in the following section and summarize the data in Table 1.
Studies of Exercise and the Immune System in Hematologic Malignancies
| Reference | Year | Study design | Hematologic malignancy | Exercise intervention | Immune component examined | Results |
|---|---|---|---|---|---|---|
| Battaglini et al103 | 2009 | Single center, prospective | Acute leukemia | Aerobic and strength exercise program 3 times per wk | IL-6. IL-10, IFN -γ | Cardiorespiratory endurance improved (P = .009, decrease in fatigue scores (P = .009), decrease in depression scores (P = .023). Trend toward significant decrease in IL-6 (P = .059); no significant changes in IL-10 (P = .223) or IFN-γ (P = .882) |
| Ladha et al104 | 2006 | Single center, prospective RCT | ALL | A single 30-min treadmill intervention to peak VO2 capacity | Neutrophil number and function | Increase in absolute neutrophil count in both exercise groups (ALL and healthy control), P = .011. Neutrophil oxidative capacity was decreased at baseline for the ALL group (P = .029) but improved with exercise |
| Perry et al100 | 2012 | Single center, prospective trial | CLL | Aerobic treadmill based exercise program | Treg, Th17-, IL-6, TGF-β, IL-2 | Exercise caused: (1) a decrease in Tregs (↓30%); (2) an increase in Th17 cells; and (3) a significant increase in the levels of IL-6 (P = .03 and TGF-β (P = .01) but not of IL-2 |
| Singh et al105 | 2005 | Murine model | T-cell lymphoma | Aerobic exercise | Macrophages, IL-1, TNF, NO | Tumor growth was reduced (P < .05). Improved survival, increased macrophage-mediated tumor cytotoxicity, and macrophage production of LPS + IFN-γ stimulated IL-1, TNF, and NO |
| Verma et al106 | 2009 | Murine model | Lymphoma | Aerobic exercise | IL-1, IL-4, IL-10, TGF-β and IFN-γ, NO, iNOS | Tumor burden and VEGF expression were reduced in a dose-dependent manner (P < .05) at 30 and 60 min postexercise. Reduced expression of IL-4 (P < .05), IL-10 (P < .05), and TGF-β but increased expression of IFN-γ and IL-1 (P < .05) |
| Zielinski et al109 | 2004 | Murine model | Lymphoma | Aerobic exercise | Macrophages and neutrophils | Delay in tumor growth, decrease in macrophages and neutrophils, decrease in tumor blood vessels (P < .006) |
| Zimmer et al102 | 2014 | Single center, prospective RTC | NHL | 30-min bicycle-based aerobic exercise | Macrophages, NK cells, CD8+ T cells, IL-6 | IL-6 was higher in the NHL patients compared with control subjects (P = .014), acetylation of the CD8+ T-cell histone H4K45 increased (P = .041) compared with control subjects |
| Reference | Year | Study design | Hematologic malignancy | Exercise intervention | Immune component examined | Results |
|---|---|---|---|---|---|---|
| Battaglini et al103 | 2009 | Single center, prospective | Acute leukemia | Aerobic and strength exercise program 3 times per wk | IL-6. IL-10, IFN -γ | Cardiorespiratory endurance improved (P = .009, decrease in fatigue scores (P = .009), decrease in depression scores (P = .023). Trend toward significant decrease in IL-6 (P = .059); no significant changes in IL-10 (P = .223) or IFN-γ (P = .882) |
| Ladha et al104 | 2006 | Single center, prospective RCT | ALL | A single 30-min treadmill intervention to peak VO2 capacity | Neutrophil number and function | Increase in absolute neutrophil count in both exercise groups (ALL and healthy control), P = .011. Neutrophil oxidative capacity was decreased at baseline for the ALL group (P = .029) but improved with exercise |
| Perry et al100 | 2012 | Single center, prospective trial | CLL | Aerobic treadmill based exercise program | Treg, Th17-, IL-6, TGF-β, IL-2 | Exercise caused: (1) a decrease in Tregs (↓30%); (2) an increase in Th17 cells; and (3) a significant increase in the levels of IL-6 (P = .03 and TGF-β (P = .01) but not of IL-2 |
| Singh et al105 | 2005 | Murine model | T-cell lymphoma | Aerobic exercise | Macrophages, IL-1, TNF, NO | Tumor growth was reduced (P < .05). Improved survival, increased macrophage-mediated tumor cytotoxicity, and macrophage production of LPS + IFN-γ stimulated IL-1, TNF, and NO |
| Verma et al106 | 2009 | Murine model | Lymphoma | Aerobic exercise | IL-1, IL-4, IL-10, TGF-β and IFN-γ, NO, iNOS | Tumor burden and VEGF expression were reduced in a dose-dependent manner (P < .05) at 30 and 60 min postexercise. Reduced expression of IL-4 (P < .05), IL-10 (P < .05), and TGF-β but increased expression of IFN-γ and IL-1 (P < .05) |
| Zielinski et al109 | 2004 | Murine model | Lymphoma | Aerobic exercise | Macrophages and neutrophils | Delay in tumor growth, decrease in macrophages and neutrophils, decrease in tumor blood vessels (P < .006) |
| Zimmer et al102 | 2014 | Single center, prospective RTC | NHL | 30-min bicycle-based aerobic exercise | Macrophages, NK cells, CD8+ T cells, IL-6 | IL-6 was higher in the NHL patients compared with control subjects (P = .014), acetylation of the CD8+ T-cell histone H4K45 increased (P = .041) compared with control subjects |
iNOS, inducible nitric oxide synthase; LPS, lipopolysaccharides; NO, nitric oxide; VEGF, vascular endothelial growth factor; VO2, oxygen consumption.
Clinical trials
Perry et al100 compared absolute numbers of regulatory T cells (Tregs) in patients with stable CLL vs CLL patients who had increased their ALCs over a 12-month period (increase of ≥30%). Patients with stable CLL had a decreased percentage of protumorigenic Tregs, suggesting a relation between Tregs and CLL progression. To determine whether exercise could affect T-cell populations and negate this relation, the authors compared 4 patients with CLL vs 4 healthy athletes in response to an acute session (45-60 minutes for CLL and 60-120 minutes for athletes) of treadmill exercise at 70% of heart rate reserve. Blood samples were collected before, immediately after exercise, and 1 hour after exercise; they were then analyzed for ALC, CD4+ Tregs, and T helper 17 (Th17) cells. Although ALC increased after exercise, numbers of CD4+ T cells were unchanged in the patients with CLL. However, the composition of CD4+ cells was altered, with Tregs reduced (↓30%) and Th17 cells increased (↑49%) 1 hour after completion of exercise. Interleukin-6 (IL-6) and transforming growth factor-β both increased immediately after exercise, whereas IL-2 was unchanged. Unfortunately, this study had inherent experimental design issues, including very small sample size, absence of a CLL control group, lack of chronic exercise training intervention, and a nonstandardized acute exercise protocol. However, it does suggest that exercise has the potential to alter the frequencies of pro-tumorigenic Treg and Th17 cells; the role of these cells is controversial, however, and not well understood.101
Zimmer et al102 enrolled 30 patients with NHL who had recently completed chemoimmunotherapy to either a control group or acute exercise intervention. Ten healthy adults were also assigned to either the control group or the exercise intervention. The intervention consisted of 30 minutes of moderate-intensity exercise on a cycle ergometer. Blood tests were conducted before the intervention and 30 minutes’ postexercise cessation. Compared with healthy control subjects, patients with NHL had higher concentrations of macrophage inhibitory factor and IL-6, whereas NK cell histone acetylation was lower, suggesting a greater pro-inflammatory environment and reduced transcriptional activity of lymphocytes. Compared with NHL control subjects, IL-6 levels were higher and acetylation of the CD8+ T-cell histone H4K45 increased in response to the exercise in patients with NHL. There were negative correlations between changes in macrophage inhibitory factor and H4K45 acetylation in the patients with NHL, suggesting an inflammatory-mediated epigenetic regulatory pathway that can be modified by acute exercise. Acute exercise seemed to beneficially alter the epigenetic pattern of NK cells and CD8+ T cells, at least in the short term. If these effects translate to long-term exercise training–induced epigenetic modifications, this will be an important step in understanding the biological mechanism of exercise training in NHL.
To examine the feasibility of an exercise intervention in patients with AML undergoing inpatient treatments, Battaglini et al103 enrolled 10 patients to receive 2 × 30-minute exercise sessions (aerobic, strength, and core) at submaximal intensities 3 times per week for 3 to 5 weeks. The main end point was feasibility, but secondary end points included physiological (eg, cardiorespiratory endurance), psychological, and systemic inflammation (IL-6, IL-10, or interferon-γ [IFN-γ]). Although lean body mass was reduced during the intervention, significant improvements were observed for cardiorespiratory fitness, fatigue, and depression. No changes were observed for inflammatory markers. Although a small study, its results show that cardiorespiratory fitness can be increased rapidly, but the biology (eg, inflammation) may need >5 weeks to change.
Ladha et al104 assessed changes in neutrophil counts and functions in four 7- to 18-year-old male subjects with acute lymphoblastic leukemia (ALL) after an acute exercise session (30-minute run/walk at 70%-80% aerobic capacity). Blood tests were conducted before, immediately after, 1 hour after, and 2 hours after exercise. The ALL group and 6 healthy control subjects had similar neutrophil kinetic responses to the exercise. Specifically, a significant increase in absolute neutrophil counts was noted from before to immediately after exercise, a decrease from immediately after exercise to 1 hour after exercise, and an increase from 1 hour after exercise to 2 hours after exercise. Oxidative burst, which is representative of antimicrobial intracellular killing, was lower at baseline in the ALL group compared with the healthy control subjects, but both groups increased after exercise. The authors were interested in whether a single session of exercise caused an impaired neutrophil response that would be reflective of a suppressed immune function, and increased risk of bacterial infection. As such, acute exercise in patients with ALL was not associated with an exercise-mediated neutrophil impairment, suggesting exercise is immunologically safe.
Animal studies
In a model of transplantable T-cell lymphoma, Singh et al105 examined the dose–response of exercise. In this study, mice were exercised at >80% of aerobic capacity for 10 consecutive days on a treadmill for various time intervals (15, 30, 60, 90, and 120 minutes per day). Compared with a control group (no exercise), tumor growth was reduced after 60, 90, and 120 minutes per day of running. Compared with findings in control mice, both 90 and 120 minutes per day of exercise were associated with improved survival, increased macrophage-mediated tumor cytotoxicity, and macrophage production of lipopolysaccharides + IFN-γ–stimulated IL-1, tumor necrosis factor, and nitric oxide. This study was one of the first to show a dose–response for exercise and possible anticancer mechanisms, including induction of tumor cell apoptosis, defective tumor cell proliferation, and augmented macrophage production of tumor-inhibiting factors.
In their follow-up study, Verma et al106 examined the tumor microenvironment of T-cell lymphoma mice after 10 days of treadmill running at either 30 or 60 minutes per day. Again, compared with control mice, tumor burden was reduced in a dose-dependent manner, which was associated with reductions in soluble vascular endothelial growth factor leading to decreased tumor angiogenesis. After exercise training, the tumor microenvironment also had a shift in the profile of Th1 to Th2 cytokines. Specifically, lower concentrations of IL-4, IL-10, and transforming growth factor-β, and increased expression of IFN-γ and IL-1, were observed. These cytokines and proportions of cytokines are important regulators of vascular endothelial growth factor–induced angiogenesis and tumor cell growth.107,108 Taken together, the research by the laboratory of Singh et al highlights the mechanistic dose–response interplays between exercise-induced modulation of immune functions and anticancer soluble factors on tumor burden in lymphoma.
In an allogeneic subcutaneous lymphoid tumor model, Zielinski et al109 assessed the tumor microenvironment after 5 to 14 days of variable (20-40 m per minute) treadmill running. Although no difference in absolute tumor volume was observed, peak tumor volume in the exercise group occurred 2 full days after the control group. Tumor regression was greater in the exercise group and associated with increased numbers of tumor-infiltrating lymphocytes at peak tumor occurrence. Interestingly, the control group had more macrophages, neutrophils, blood vessels, and apoptotic bodies than the exercise group, suggesting that exercise had successfully altered the tumor-immune kinetics. Taken together, animal studies offer a unique insight into the mechanisms by which exercise can modulate the immune system in hematologic malignancies.
In conclusion, exercise has the potential to improve a range of outcomes in patients with hematologic cancer. Reviewing the literature in hematologic malignancies found that small studies show improved outcomes in areas such as QoL and fatigue, but larger randomized trials are needed to better understand the benefits of exercise. Furthermore, immune modulation observed with exercise in healthy individuals illustrates one potential avenue that exercise could be beneficial in hematologic malignancies. Due to the inherent dysfunction of both the underlying hematologic malignancy cell and the microenvironment of the tumor cells (eg, T cell, NK cell dysfunction),110 it stands to reason that the positive outcomes associated with exercise and hematologic malignancy may be associated with the immune impact of exercise. These potentially relate to both mobilization of cells as well as augmentation in function as seen in the small trials outlined here. Although the discussed studies are too small to make significant conclusions, they certainly show potential areas for further exploration, particularly regarding NK cells, T cells, macrophages, and neutrophil function.
In terms of exercise in immunocompromised hematologic patients, the issue of safety and possible deleterious effects of “too much” exercise often arises. Campbell and Turner41 discuss how exercise actually results in an acute “heightened” immune surveillance that occurs 1 to 2 hours after exercise, rather than immunosuppression. They also highlight how vaccine response is improved in active older adults who regularly exercise (generally >60 years of age) vs sedentary adults, and thus exercise may actually lessen the aging of the immune system. In a small study of patients undergoing adult allogenic stem cell transplantation, exercise was shown to have no additional risks to the patient during this highly vulnerable immunocompromised state but did improve endurance (P = .002), muscular strength (P = .022), fatigue (P = .046), and emotional well-being (P = .028).111 Although there are a myriad of factors to consider regarding exercise in an individual patient with hematologic malignancies, worsening immunosuppression is unlikely and may actually be improved.
Finally, the available research highlights several future areas of research interest. First, larger studies similar to those in solid malignancies are needed to show the impact of exercise on clinical outcomes such as symptoms, QoL, and overall survival in hematologic malignancies. To this end, there are 4 actively recruiting exercise trials in adult hematologic malignancies that we know of that are not transplant related, although none are multi-site RCTs (NCT04052126, NCT04057443, NCT03923504, and NCT03953326). Second, the mechanisms of how exercise improves outcomes need to be elucidated. This information will allow us to most effectively use exercise as an adjuvant to prevention and treatment. Given that data from exercise in healthy individuals show a significant impact on the immune system, and a few small studies in hematologic malignancies suggest this association, the immunomodulation effects of exercise are of particular interest. Moreover, the current treatment landscape, which increasingly emphasizes immunotherapies and harnessing the immune system, makes the intersection of exercise and the immune system in hematologic malignancies even more interesting as a potential adjunct to treatment and hematologic malignancy care. With a better understanding of how exercise mechanistically affects the immune system and clinical outcomes in hematologic malignancy, exercise could eventually be “prescribed” to better augment treatment, prevention, and patient outcomes.
All data requests should be submitted to the corresponding author, Andrea Sitlinger (andrea.sitlinger@duke.edu).
Acknowlegdments
This work was supported by a National Institutes of Health, National Heart, Lung, and Blood Institute T32 grant (T32HL007057) and the Duke Claude D. Pepper Older Americans Independence Center Pilot Study Award (National Institutes of Health, National Institute on Aging P30-AG028716).
Authorship
Contribution: A.S. performed the literature review, analysis and writing of the manuscript; and D.M.B. and D.B.B. equally contributed to providing additional analysis and significant edits/writing of the manuscript.
Conflict-of-interest disclosure: D.M.B. has been a consultant, scientific advisory board member, and site clinical trial Principal Investigator (PI) (grant paid to institution) for AbbVie, Genentech, and Verastem; scientific advisory board member and site clinical trial PI (grant paid to institution) for ArQule and TG Therapeutics; site clinical trial PI (grant paid to institution) for Ascentage, BeiGene, DTRM, Juno/Celgene/BMS, MEI Pharma, and Tolero; consultant and site clinical trial PI (grant paid to institution) for AstraZeneca and Pharmacyclics; consultant and scientific advisory board member for Pfizer; consultant for Teva; National Comprehensive Cancer Network panel member; and has participated in the informCLL registry steering committee (AbbVie), REAL registry steering committee (Verastem), and Biosimilars outcomes research panel (Pfizer). The remaining authors declare no competing financial interests.
Correspondence: Andrea Sitlinger, Duke University School of Medicine, 20 Duke Medicine Cir, Durham, NC 27710; e-mail: andrea.sitlinger@duke.edu.

