

Key Points
ADAMTS13 activities may serve as biomarkers to guide caplacizumab treatment modalities and overall treatment duration.
von Willebrand factor activities may be used for therapeutic drug monitoring of caplacizumab.

Abstract
Introduction of the nanobody caplacizumab was shown to be effective in the treatment of acquired thrombotic thrombocytopenic purpura (aTTP) in the acute setting. The official recommendations include plasma exchange (PEX), immunosuppression, and the use of caplacizumab for a minimum of 30 days after stopping daily PEX. This study was a retrospective, observational analysis of the use of caplacizumab in 60 patients from 29 medical centers in Germany. Immunosuppressive treatment led to a rapid normalization of ADAMTS13 activities (calculated median, 21 days). In 35 of 60 patients, ADAMTS13 activities started to normalize before day 30 after PEX; in 11 of 60 patients, the treatment was extended beyond day 30; and in 5 patients, it was extended even beyond day 58 due to persistent autoimmune activity. In 34 of 60 instances, caplacizumab was stopped before day 30 with a favorable outcome whenever ADAMTS13 activities were >10%. In contrast, 11 of 34 patients with ADAMTS13 activities <10% at the time of stopping caplacizumab treatment developed a nonfavorable outcome (disease exacerbation or relapse). In some cases, prolongation of the treatment interval to every other day was feasible and resulted in a sustained reduction of von Willebrand factor activity. ADAMTS13 activity measurements are central for a rapid diagnosis in the acute setting but also to tailor disease management. An ADAMTS13 activity–guided approach seems safe for identifying the individual time point when to stop caplacizumab to prevent overtreatment and undertreatment; this approach will result in significant cost savings without jeopardizing the well-being of patients. In addition, von Willebrand factor activity may serve as a biomarker for drug monitoring.
Introduction
The advent of the anti–von Willebrand factor (VWF) humanized nanobody caplacizumab has broadened the therapeutic armamentarium for treating acute episodes of acquired thrombotic thrombocytopenic purpura (aTTP). However, real-world safety and efficacy outside of expert centers, effect of cost on utilization, adherence in nonclinical trials, and optimal duration of therapy are unknown.1 The high costs (on average, US$270 000 per course) might also limit its use. A retrospective, observational analysis2 on the use of caplacizumab during acute disease management in 60 patients from 29 medical centers in Germany from June 2018 to December 2019 confirmed the drug’s therapeutic potential as described in 2 double-blind controlled trials; this led to the rapid approval of the drug in Europe and the United States.3,4 In the German cohort, treatment modalities were very heterogeneous. Caplacizumab was used as front-line treatment in 35 (58.3%) of 60 patients. In this real-world cohort, caplacizumab led to a rapid normalization of the platelet count in all patients as reported in the TITAN (phase 2) and HERCULES (phase 3) trials.3,4 This effect was very robust and was observed in patients in whom caplacizumab was used early in treatment as well as in cases of refractory disease. The delayed use of caplacizumab in a significant proportion of patients resulted in a higher need of plasma exchange (PEX) (11.8 days vs 5.8 days in HERCULES), prolonged hospitalization (21.6 days vs 9.9 days), and 1 death related to aTTP-associated complications. After the start of caplacizumab, however, only a median of 4 additional PEX were necessary, again confirming the published results from the HERCULES trial. Moreover, recent reports have described PEX-free treatment regimens of acute episodes of aTTP with caplacizumab with an overall favorable outcome.5,6 With this growing body of evidence, caplacizumab has become more and more widely accepted and is recommended as front-line treatment for acute episodes of aTTP.
Official recommendations for the use of caplacizumab follow the therapeutic scheme from the HERCULES trial.4 In addition to an initial intravenous dose before PEX, daily subcutaneous injections following PEX are recommended for an additional 30 days after PEX is stopped. The guidelines also recommend extending the treatment duration if ADAMTS13 activity remains <10% thereafter. These recommendations remain a matter of an ongoing scientific debate as no pathophysiological or clinical justification has been reported for a fixed treatment period >30 days after stopping PEX. On the contrary, a prolongation in cases of persistent autoimmune activity seems justified, although the exact length of the treatment extension must be better defined.3 In HERCULES, patients experienced a disease relapse after stopping caplacizumab 58 days after the last PEX, most likely due to persistent autoantibodies and reduced ADAMTS13 activities.4 With the increasing availability of caplacizumab, reliable markers for treatment success and identification of laboratory and/or clinical landmarks to control treatment should be quickly established.
Given its central role in the pathogenesis of aTTP, ADAMTS13 activity measurements have gained much interest not only for a rapid diagnosis in the acute setting but also to tailor disease management.7-11 An ADAMTS13-guided approach may enable physicians to identify the individual time point when to stop caplacizumab to prevent overtreatment and undertreatment. This action may also result in significant cost savings without jeopardizing the well-being of patients with aTTP. The current article provides a comprehensive analysis of the treatment modalities of the first 60 patients treated with caplacizumab in Germany, infers strategies to reduce caplacizumab doses by using VWF activity as a biomarker for drug monitoring, and offers an analysis of cost-saving potential.
Methods
Study design and participants
This study was conducted as a retrospective, observational analysis at 29 German medical centers. In total, 60 patients with aTTP were identified who received caplacizumab between June 2018 and December 2019. Time to final recovery of ADAMTS13 activity was defined as the time to the first day with a measurement ≥10% that was not followed by another measurement below this value unless this was deemed due to a late relapse unrelated to the previous episode. ADAMTS13 activity measurements with ongoing PEX were excluded. Time to normalization of platelet count after caplacizumab treatment start was defined as the first day with a count ≥150 × 10E9/L.
If caplacizumab treatment was stopped and resumed later due to exacerbation or relapse, time to normalization was measured again (as in cases #3, #28, #33, #38, #42, #43, and #57). Clinical remission, exacerbation, refractory disease, and relapse were defined as published previously, with the exception that re-initiation of PEX was not a prerequisite of exacerbation and relapse because some of these instances were managed with conservative treatment only.12 Treatment according to the HERCULES protocol was defined as caplacizumab initiated before or after the first PEX and continued for a minimum of 30 days and a maximum of 58 days after the last PEX treatment. Treatment decisions were interpreted according to the reported laboratory parameters and therapeutic interventions. In case of uncertainties regarding the rationale, treating physicians were contacted in person, by telephone, or by e-mail to clarify their decision-making process.
VWF activity measurements
VWF activity measurements were performed at the respective centers. The INNOVANCE-VWF-AC reagent (Siemens Healthcare Diagnostics, Erlangen, Germany) on the Sysmex CS-5100, Atellica COAG 360 platform, was used in all instances.
Analysis of cost-saving potential
The global cost-saving analysis comprises 3 independent calculations. First, we calculated the number of doses that were saved by stopping caplacizumab treatment successfully, guided according to either platelet count or ADAMTS13 activity, before completing 30 doses after PEX (following the HERCULES study protocol). Instances in which this procedure resulted in an exacerbation or relapse were not considered, and additional potential costs arising from intensified treatment after unsuccessful attempts to stop caplacizumab were not calculated. Second, the number of doses saved by successfully switching patients to a nondaily administration regimen was calculated. The total number of days on caplacizumab after PEX was compared vs the actual number of doses administered to the patient every other day. Third, we calculated the predicted number of doses that could have been saved if caplacizumab treatment had been stopped on the day of the first ADAMTS13 activity measurement >10% after PEX (ie, the consistent use of ADAMTS13 activities to guide caplacizumab therapy duration). To calculate total cost savings, hypothetical saved doses were multiplied by €5660 or US$7660 as the marketing prices in Germany and the United States, respectively, as of October 2019.
The individual caplacizumab dose and cost calculation involved 3 main strategies. First, the calculation of hypothetical doses if a particular treatment had either been guided by: (1) the official registration information of caplacizumab in the United States (ie, the HERCULES protocol), (2) an ADAMTS13 activity–guided approach, and (3) an ADAMTS13 activity–guided approach with alternate-day dosing after the end of PEX treatment. Second, a cost calculation of each individual patient was provided based on the actual treatment modalities (“real-world data”). Based on this real-world evidence gathered herein, we report the actual doses per patient and calculate saved caplacizumab doses for those patients who: (1) have not completed 30 days of caplacizumab post-PEX based on ADAMTS13 activity, (2) have not completed 30 days of caplacizumab post-PEX based on platelet counts, or (3) have been switched to a nondaily dosing regimen post-PEX. If stopping caplacizumab before day 30 post-PEX led to an exacerbation or relapse, the estimated costs of additional rituximab, ICU days, and PEX are also reported. Third, we report the real-world data of total costs of conventional treatment (rituximab, ICU days, and PEX). More details regarding the calculation are given in the legend of Table 3 and supplemental Table 2.13,14
Statistical analysis
Given the exploratory nature of the current study, no sample size calculation and no adjustments for multiple testing were performed. All results are given as median (interquartile range) or mean with 95% confidence interval (CI) when appropriate. For the linear regression analysis, the Mann-Whitney U test was used to determine statistical significance. Statistical analysis was conducted by using GraphPad Prism version 8.0.1 (GraphPad Software, San Diego, CA). Figures and tables were designed and composed by using Microsoft Office (Microsoft Corp, Redmond, WA) and Adobe Illustrator (Adobe Systems Software Ireland Ltd, Dublin, Ireland).
Results
Individual patient characteristics, treatment modalities, and individual courses comprising platelet counts and ADAMTS13 activity measurements and therapeutic interventions are reported in supplemental Table 1 and supplemental Figure 1 and are described in detail by Voelker et al.2
ADAMTS13 activity as a biomarker to guide treatment modalities
ADAMTS13 activities were regularly assessed during caplacizumab treatment in 45 (75.0%) of 60 patients. The median time after diagnosis to final ADAMTS13 activity recovery to >10% was 32.5 (8-204) days and 21 (1-191) days after stopping PEX treatment (Figure 1). Thirty-five (58.3%) of 60 patients reached ADAMTS13 activities >10% before day 30 after stopping PEX (median, 21 days; range, 1-191 days). In a linear regression analysis, patients with a first episode of aTTP took significantly less time to resolve autoimmune activity and restore ADAMTS13 activity compared with patients with recurrent disease. No other parameter was identified to significantly correlate with time to ADAMTS13 activity recovery; in particular, sex and body mass index had no effect (Table 1).
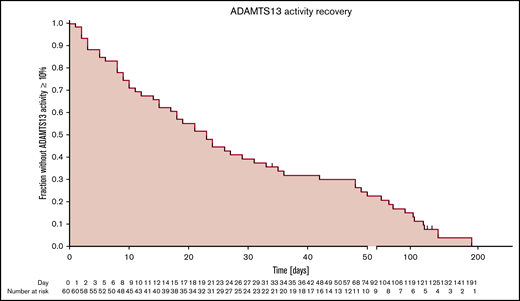
Kaplan-Meier curves of patient fractions remaining without ADAMTS13 activity (>10%) recovery after the end of PEX treatment.
Kaplan-Meier curves of patient fractions remaining without ADAMTS13 activity (>10%) recovery after the end of PEX treatment.
Outcomes data
| Variable | Germany (n = 60) | Statistical significance (Mann-Whitney U test) |
|---|---|---|
| Time to final ADAMTS13 activity recovery >10% after diagnosis, median, d (IQR) | 32.5 (21-53) | |
| Reached at end of follow-up, % (n/N) | 90.0 (54/60) | |
| Not reached at end of follow-up, % (n/N) | 10.0 (6/60) | |
| Time to final ADAMTS13 activity recovery >10% after end of PEX, median, d (IQR) | 21 (9-48) | |
| Reached at end of follow-up, % (n/N) | 90.0 (54/60) | |
| Not reached at end of follow-up, % (n/N) | 10.0 (6/60) | |
| Linear regression of time to final ADAMTS13 activity recovery >10% after end of PEX | ||
| Patients with first episode of aTTP (n = 46) | P = .046 for difference between groups | |
| Median, d (IQR) | 18.0 (8.0-35.3) | |
| Mean, d (SD) | 29.3 (36.9) | |
| Patients with recurrent aTTP, median (n = 14) | ||
| Median, d (IQR) | 45.5 (12.5-109.7) | |
| Mean, d (SD) | 61.4 (51.0) | |
| Female patients (n = 42) | P = .923 for difference between groups | |
| Median, d (IQR) | 21 (8.8-48.0) | |
| Mean, d (SD) | 35.2 (38.6) | |
| Male patients (n = 18) | ||
| Median, d (IQR) | 21 (3.0-55.3) | |
| Mean, d (SD) | 40.6 (51.4) | |
| Body mass index ≤24 kg/m2 (n = 13) | P = .742 for difference between groups | |
| Median, d (IQR) | 23.0 (6.5-33.5) | |
| Mean, d (SD) | 23.1 (16.1) | |
| Body mass index >24 kg/m2 (n = 46) | ||
| Median, d (IQR) | 18.0 (8.8-51.0) | |
| Mean, d (SD) | 38.9 (45.6) |
| Variable | Germany (n = 60) | Statistical significance (Mann-Whitney U test) |
|---|---|---|
| Time to final ADAMTS13 activity recovery >10% after diagnosis, median, d (IQR) | 32.5 (21-53) | |
| Reached at end of follow-up, % (n/N) | 90.0 (54/60) | |
| Not reached at end of follow-up, % (n/N) | 10.0 (6/60) | |
| Time to final ADAMTS13 activity recovery >10% after end of PEX, median, d (IQR) | 21 (9-48) | |
| Reached at end of follow-up, % (n/N) | 90.0 (54/60) | |
| Not reached at end of follow-up, % (n/N) | 10.0 (6/60) | |
| Linear regression of time to final ADAMTS13 activity recovery >10% after end of PEX | ||
| Patients with first episode of aTTP (n = 46) | P = .046 for difference between groups | |
| Median, d (IQR) | 18.0 (8.0-35.3) | |
| Mean, d (SD) | 29.3 (36.9) | |
| Patients with recurrent aTTP, median (n = 14) | ||
| Median, d (IQR) | 45.5 (12.5-109.7) | |
| Mean, d (SD) | 61.4 (51.0) | |
| Female patients (n = 42) | P = .923 for difference between groups | |
| Median, d (IQR) | 21 (8.8-48.0) | |
| Mean, d (SD) | 35.2 (38.6) | |
| Male patients (n = 18) | ||
| Median, d (IQR) | 21 (3.0-55.3) | |
| Mean, d (SD) | 40.6 (51.4) | |
| Body mass index ≤24 kg/m2 (n = 13) | P = .742 for difference between groups | |
| Median, d (IQR) | 23.0 (6.5-33.5) | |
| Mean, d (SD) | 23.1 (16.1) | |
| Body mass index >24 kg/m2 (n = 46) | ||
| Median, d (IQR) | 18.0 (8.8-51.0) | |
| Mean, d (SD) | 38.9 (45.6) |
N with available data as indicated.
IQR, interquartile range presented as quartile 1 and quartile 3 cutoff value; SD, standard deviation.
Caplacizumab was stopped before day 30 in 35 instances in 31 of 60 patients (Table 2). Of note, in 4 cases (cases #3, #24, #28, and #38), caplacizumab was stopped twice before completion of a full course of 30 doses. Case #18 was excluded from this analysis due to the fatal outcome. In 20 of these instances, a platelet count–guided approach (ie, thrombocytes >150 × 10E9/L) was used to halt caplacizumab treatment. In 45% (9 of 20) of such instances, the patients experienced a disease exacerbation. In 15 additional instances, treatment was terminated before day 30 based on restored ADAMTS13 activities. None of these patients developed signs of exacerbation or early relapse during the follow-up period. In 11 of the reported 60 patients, treatment was extended beyond day 30 due to low ADAMTS13 activities. In one of these patients (#33), caplacizumab was extended beyond day 30 in 2 instances. In a total of 12 instances in these 11 patients, treatment was extended by an average of 80.6 days (95% CI 55.9-105.3) post-PEX. No patient with ADAMTS13 activity >10% at the time of stopping caplacizumab treatment experienced an exacerbation or relapse within the observation period. In contrast, 11 of 34 patients with ADAMTS13 activities <10% at the time of stopping caplacizumab treatment developed a nonfavorable outcome (ie, disease exacerbation or relapse) (Figure 2). Of note, 10 of 11 events occurred within the first 4 weeks after stopping PEX, and all events occurred within 15 days after stopping caplacizumab (mean, 6.9 days; 95% CI, 3.9-9.9).
Instances of early (<30 days post-PEX) termination of caplacizumab treatment stratified according to outcome (ie, nonsuccessful [exacerbation, relapse, or death] vs successful [no such event])
| Approach | Successful | Nonsuccessful |
|---|---|---|
| ADAMTS13 guided | 15 | 0 |
| Platelet count guided | 11 | 9 |
| Total | 26 | 9 |
| Approach | Successful | Nonsuccessful |
|---|---|---|
| ADAMTS13 guided | 15 | 0 |
| Platelet count guided | 11 | 9 |
| Total | 26 | 9 |
An ADAMTS13-guided approach was assumed when a (rising) ADAMTS13 activity >10% was known to the treating physicians at the time of stopping caplacizumab. A platelet count–guided approach was assumed when no such activity measurement was known or activity was still <10% at the time of stopping caplacizumab.
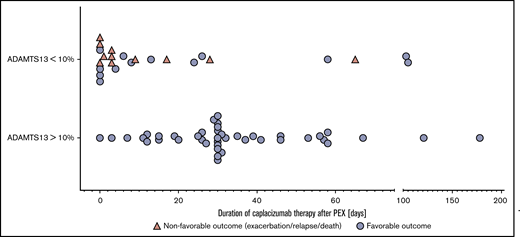
Duration of caplacizumab treatment after end of PEX in relation to outcome. Caplacizumab treatment duration after PEX stratified according to ADAMTS13 activity at the time of stopping caplacizumab. Nonfavorable outcomes include exacerbation, relapse, and death. Two cases were censored due to ongoing caplacizumab treatment and registered as being in remission at the time point of the census. It is noteworthy that in 6 cases, >1 instance of termination of caplacizumab treatment after PEX was reported. Days of caplacizumab treatment do not necessarily reflect the doses of caplacizumab because some patients were treated with a nondaily or intermittent caplacizumab regimen.
Duration of caplacizumab treatment after end of PEX in relation to outcome. Caplacizumab treatment duration after PEX stratified according to ADAMTS13 activity at the time of stopping caplacizumab. Nonfavorable outcomes include exacerbation, relapse, and death. Two cases were censored due to ongoing caplacizumab treatment and registered as being in remission at the time point of the census. It is noteworthy that in 6 cases, >1 instance of termination of caplacizumab treatment after PEX was reported. Days of caplacizumab treatment do not necessarily reflect the doses of caplacizumab because some patients were treated with a nondaily or intermittent caplacizumab regimen.
Supplemental Table 1 lists the modifications of the immunosuppressant regimen that have been introduced after 30 days of protracted autoimmune activity in the 15 patients in the upper quartile with the longest time to ADAMTS13 activity normalization after PEX (equal to ≥54 days after PEX). Additional immunosuppressive medications were introduced in 7 (46.7%) of 15 patients and comprised mycophenolate, azathioprine, increased doses of rituximab, and cyclosporine.
There is evidence that front-line rituximab treatment within 72 hours after disease onset is superior to later treatment, with faster attainment of remission and normalization of ADAMTS13 activity.15 In this cohort, 48 (80.0%) of 60 patients were treated with 1 to 6 doses of rituximab, with a median cumulative dose of 2000 mg (562.5-5000 mg). On average, patients received the first dose of rituximab on day 7 (0-26 days). In 11 (18.3%) of 60 patients, rituximab was used as a front-line agent. Surprisingly, the use of rituximab either as front-line therapy within 72 hours after starting the specific treatment or later had no impact on ADAMTS13 normalization (log-rank test, not significant; χ2 test, 2.563 [P = .278]; log-rank test for trend, not significant; χ2 test, 1.150 [P = .284]). We also analyzed the impact of the inhibitory autoantibody and antigen levels, remaining ADAMTS13 activity, and organ damage markers at presentation (lactate dehydrogenase, troponin, creatinine, and Glasgow Coma Scale) on ADAMTS13 recovery but observed no significant correlations.
VWF activity–based therapeutic drug monitoring of caplacizumab
Based on the published pharmacokinetic parameters of caplacizumab, 10 patients (cases #24, #29, #33, #34, #36, #37, #43, #44, #47, and #50) were given a nondaily caplacizumab regimen ranging from alternate-day to once weekly schedules and were closely monitored for signs of disease activity.3 In 6 of these 10 cases, repeated measurements of VWF activity were conducted, which revealed therapeutic inhibition over 48 hours (Figure 3). In patients #29, #33, and #43, the dosing intervals were extended to an alternate-day dosing regimen immediately after cessation of PEX. In patient #34, VWF activity levels were >10% on days 1 and 2 after PEX, and the dosing interval was first extended on day 3 after PEX when VWF activity was no longer detectable. Patients #36 and #37 were started on a daily caplacizumab regimen and switched to alternate dosing intervals after 2 or 6 days, respectively. In the 4 patients without repeated VWF activities (#24, #44, #47, and #50), the treatment regimen in one (#24) did not follow a particular dosing schedule but seemed to be primarily guided by the day-to-day dynamic of the platelet count. However, no deliberate attempt to elongate the dosing interval was made. In the other instances (#44, #47, and #50), the patients were switched to an alternate-day dosing regimen when ADAMTS13 became detectable (#44) or 1 week after the ADAMTS13 activity had recovered and platelet counts had stabilized. The caplacizumab treatment was stopped after an additional 19, 15, or 7 days (#44, #47, and #50). On a cautionary note, however, 3 instances of a drop in platelet count on an alternate-day caplacizumab dosing regimen in 2 patients were observed. These instances were asymptomatic, did not entail a rise in organ damage markers, and could be managed by reverting to daily caplacizumab dosing for a short period of time. In one patient (#58), 2 consecutive caplacizumab doses in the early phase of the treatment were accidentally omitted when platelet counts were already increasing. This patient developed a prolonged phase of severe refractoriness.
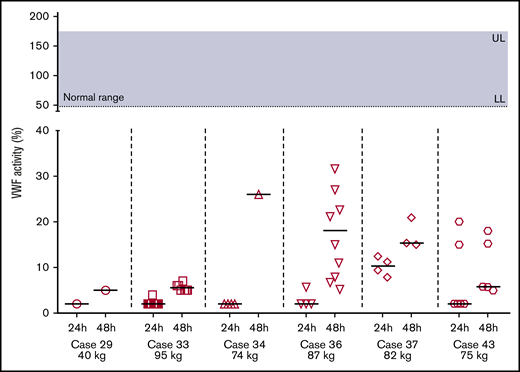
VWF activity as measured by a VWF:GP1bM activity assay on the first and second day after caplacizumab administration. Patients were on an alternate-day caplacizumab treatment regimen and closely monitored for signs of relapse. Normal range for VWF activity, 50% to 187%. LL, lower limit of normal; UL, upper limit of normal.
VWF activity as measured by a VWF:GP1bM activity assay on the first and second day after caplacizumab administration. Patients were on an alternate-day caplacizumab treatment regimen and closely monitored for signs of relapse. Normal range for VWF activity, 50% to 187%. LL, lower limit of normal; UL, upper limit of normal.
Cost-saving potential
This study used a multimodal cost analysis, as indicated in the Methods section and the legend to supplemental Table 2.13,14 A global analysis summarizes the cost-saving potential of different approaches to caplacizumab treatment guidance for all 60 patients (ie, ADAMTS13 activity-guided, platelet count-guided, and nondaily dosing regimens) (Table 3). The number of saved doses by ADAMTS13 activity guidance or platelet count guidance was calculated for those patients/instances in which caplacizumab was successfully stopped before day 30. Caplacizumab was stopped before day 30 in 35 instances (n = 31 patients [4 patients had 2 instances]). This resulted in an estimated saving of 440 doses of caplacizumab, approximating €2 490 400/US$3 388 000.
Cost-saving strategies
| Dose reduction strategy | No. of instances calculated | No. of saved doses | Cost savings, € | Cost savings, US$ |
|---|---|---|---|---|
| Real-world data: early successful termination (platelet count guided/ADAMTS13 guided) of caplacizumab treatment | 26/60 | 440 | 2 490 400 | 3 388 000 |
| Real-world data: nondaily treatment regimens* | 10/60 | 386 | 2 184 760 | 2 972 200 |
| Hypothetical model: ADAMTS13 guidance of caplacizumab treatment duration† | 29/60 | 419 | 2 371 540 | 3 226 300 |
| Dose reduction strategy | No. of instances calculated | No. of saved doses | Cost savings, € | Cost savings, US$ |
|---|---|---|---|---|
| Real-world data: early successful termination (platelet count guided/ADAMTS13 guided) of caplacizumab treatment | 26/60 | 440 | 2 490 400 | 3 388 000 |
| Real-world data: nondaily treatment regimens* | 10/60 | 386 | 2 184 760 | 2 972 200 |
| Hypothetical model: ADAMTS13 guidance of caplacizumab treatment duration† | 29/60 | 419 | 2 371 540 | 3 226 300 |
Real-world data and hypothetical cost-saving analysis investigating different dose reduction strategies in the German cohort in the post-PEX treatment period. Real-world data were based on the dose reduction strategies used by the treating physicians. The hypothetical model investigates the potential savings if this strategy had been applied to all patients in the cohort. Please note that these strategies are off-label and must be based on shared decision-making with the patient. Cost calculations are estimations based on the market price (January 2020) of €5660 per dose and US$7700 per dose. Dose reduction strategies overlap in parts and cannot be considered complementary.
Nondaily regimens ranged from alternate-day to once a week and may not be suitable for every individual or situation. VWF measurements may help identify suitable patients.
The hypothetical model assumes that no exacerbation/relapse occur after ADAMTS13-guided termination of caplacizumab treatment. Although this might be inferred from the cohort presented herein (no exacerbation/relapse in 14 of 14 attempts to stop caplacizumab treatment when ADAMTS13 activity has risen >10%), no prospective randomized data to support this idea are available.
Nondaily dosing after PEX was used in 10 patients. The number of saved doses was calculated by subtracting the actual doses from the number of daily doses that patient would have received on a daily dosing regimen. In 10 patients, nondaily dosing of caplacizumab saved ∼386 daily doses (€2 184 760/US$2 972 200).
We next determined how many doses would have been saved if caplacizumab had been stopped in all patients with an ADAMTS13 activity >10% before day 30 after PEX. In 29 of 60 patients, caplacizumab treatment was continued despite ADAMTS13 activities >10%. In this hypothetical calculation, the early termination of caplacizumab treatment would have saved 419 doses (€2 371 540/US$3 226 300).
Additional calculations of cost-saving strategies per patient are given in supplemental Table 2.13,14 Here, we calculated the actual cost of caplacizumab treatment (“as treated”) and the conventional treatment modalities (rituximab, ICU days, and PEX). In cases of an unsuccessful use of a cost-saving strategy, the cost to treat the resulting exacerbation/relapse was also estimated (as outlined in the figure legend). Due to the strong hypothetical nature of these calculations, we abstained from summarizing results but rather report individual data to elucidate cost effects of treatment decisions in individual patients.
Discussion
With the increasing use of caplacizumab in the treatment of aTTP comes the necessity to tailor treatment modalities to the individual patient beyond well-standardized clinical trial settings. To prevent undertreatment and overtreatment, as well as to alleviate the socioeconomic burden, we performed a comprehensive analysis of the first 60 patients treated with caplacizumab in Germany. The results emphasize the importance of regular measurements of ADAMTS13 activities after PEX has been stopped and to discontinue caplacizumab treatment once ADAMTS13 activity increases to >10%. In patients with persistent autoimmune activity, a treatment extension for a total of 58 days according to the HERCULES protocol seems justified to overcome the initial period of maximal vulnerability. In addition, VWF activity may prove useful as a biomarker for therapeutic drug monitoring of caplacizumab, allowing extension of the treatment interval and cost-savings without jeopardizing the patients’ well-being.
The pathophysiological hallmark of aTTP is the reduction of ADAMTS13 activity mediated by autoantibodies against ADAMTS13. Its measurement is of central importance in confirming the clinical diagnosis of aTTP. At the same time, ADAMTS13 autoantibodies and activities can be used to identify patients at risk for disease exacerbations and relapses in the weeks and months after an acute episode. In the German cohort, the median time after diagnosis to final ADAMTS13 activity recovery to >10% was 32.5 days and 21 days after stopping PEX treatment. This observation confirms results from the HERCULES trial in which 26 of 65 (40%) patients reported ADAMTS13 activities >10% in the week after the last PEX and 17 of 60 (72%) patients at the end of the caplacizumab treatment period. In HERCULES, no patient with ADAMTS13 activity >10% at the end of the treatment period experienced a disease relapse, and only 3 of 30 in the placebo group experienced an exacerbation if the ADAMTS13 activity was >10% after the last PEX.4 We made similar observations in this cohort. Recurrent aTTP was identified as a statistically significant parameter that correlated with a prolonged time to normalization of ADAMTS13 activities. These data suggest that ADAMTS13 activity starts to normalize before day 30 and that it is highly unlikely that exacerbation or relapse will occur with ADAMTS13 levels >10% on adequate immunosuppression. As a consequence, ADAMTS13 activities should be monitored closely while administering caplacizumab, and efforts should be made to improve its immediate availability.
ADAMTS13 activity measurements are essential in the diagnosis of aTTP, and monitoring seems to be promising for guiding treatment decisions regarding duration and cotreatment. We therefore advocate that ADAMTS13 activity measurements be available within hours on a nationwide basis. It is of strong interest that new tests become available that allow the rapid and fully automated measurement of ADAMTS13 activity.16 We recommend monitoring ADAMTS13 activity closely after termination of PEX and stopping caplacizumab when activity rises >10%. Repeated measurements at least 1 to 2 times per week resulted in a significant reduction of the total administered dosage of caplacizumab. In addition, nondaily administration of caplacizumab after PEX in patients with a low body weight might help to further reduce total expenses; there is a small risk of a disease exacerbation, however. Therefore, close monitoring of the platelet count is necessary when choosing such an approach. Direct measurements of VWF activity as a pharmacodynamic marker may be beneficial to identify suitable candidates as well as for therapeutic drug monitoring. Extending the treatment interval is also an important option in patients who experience side effects but are still depending on caplacizumab treatment for disease control. It must be emphasized that all such modifications should be based on broad agreement of clinicians and patients.
In many patients, we observed an excessive platelet count response ∼10 days after the start of caplacizumab treatment, which was followed by a drop of up to 30% to 40% between days 15 and 20 before reaching the individual normal levels. This dynamic thrombocyte response was not accompanied by an increase in lactate dehydrogenase or clinical signs of recurrent aTTP activity (supplemental Figure 12 ). It most likely reflects increased thrombopoiesis in response to the underlying disease and the use of high-dose glucocorticoids. As a consequence, it remains clinically challenging to differentiate this observed drop in platelet count from a potential disease exacerbation. Additional markers of hemolysis (eg, lactate dehydrogenase, haptoglobin), as well as clinical symptoms, might help to guide clinical decisions.
The autoimmune activity persisted in 11 patients, and caplacizumab treatment was extended beyond day 30. In comparison, in HERCULES, 20 of 73 patients were treated for >30 days. In detail, 2 patients had 1 week of treatment extension, 4 patients for 2 weeks, 5 patients for 3 weeks, and 9 patients for 4 weeks. The HERCULES study was funded by Ablynx, Zwijnaarde, Belgium, a Sanofi company. ClinicalTrials.gov identifier: NCT02553317; internal study number: ALX0681-C301. The study started in 2015 and ended in 2017. Although caplacizumab treatment had to be stopped in all patients after a maximum of 58 days in HERCULES, the treatment was prolonged beyond 58 days in 6 instances (cases #20, #24, #33, #34, and #36). Patient #33 experienced a relapse after 65 days (ie, 7 days after stopping caplacizumab). The patient was treated again for another 105 days until ADAMTS13 activities began to normalize.
The first weeks after cessation of PEX remain critical, particularly in patients with persistent autoimmune activity, and they justify a treatment extension. However, one might consider cessation of caplacizumab treatment in these high-risk patients after day 58 under close surveillance. In 5 of 6 incidences (1 case [#20] had insufficient data), treatment was extended due to persistent autoimmune activity. In this extended treatment subgroup, 2 instances of relapsing disease were documented, which could be detected early and could be managed by conservative treatment with no need for additional PEX. Of note, all exacerbations and relapses occurred within 2 weeks after stopping caplacizumab, again reproducing the observations described in the HERCULES trial in which all 9 subjects in the caplacizumab group with maximum treatment extension duration permitted per protocol exhibited suppressed ADAMTS13 activity at the time treatment was stopped. Four of these 9 individuals developed a relapse within 8 days after receiving the last dose of caplacizumab (Sanofi, data on file, shared by the company). Hence, it seems reasonable to stop caplacizumab treatment after 58 days even in patients with persistently low ADAMTS13 activities and high autoantibody titers under close surveillance. In case of a disease relapse, we recommend restarting caplacizumab and consideration of additional immunosuppression. However, one may also extend caplacizumab treatment until autoimmune activity has resolved. In this case, an intensification of immunosuppression ought to be considered, but no randomized data support any specific therapy or dosing regimen in this context.
Rituximab has been shown to improve the response rates in aTTP and increase relapse-free survival, particularly in patients experiencing disease relapses. Two studies argue in favor of adding rituximab early in the course of acute aTTP to reduce PEX and hospitalization.17,18 One might speculate whether its front-line use in the era of caplacizumab will help to overcome the autoimmune activity and lead to a more rapid normalization of ADAMTS13 activities. In the current cohort, 20% of all patients received rituximab within the first 72 hours and 60% later during the course of disease. Due to the retrospective nature of the study and a potential immortal time bias, we were unable to quantify the effect of rituximab on the time of ADAMTS13 activity normalization. Furthermore, any analysis might be biased by the fact that physicians tended to withhold rituximab in cases of rapidly waning thrombotic microangiopathy and potentially milder courses or administer it primarily to patients with refractory disease or exacerbation. The fact that we were unable to identify predictive factors of ADAMTS13 activity recovery except the presence of a first episode of aTTP argues for front-line use of rituximab or other immunosuppressant agents in all patients; this is important because which patients will exhibit protracted autoimmune activity remains unpredictable at the time of disease onset. Why autoimmune activity in patients with recurrent aTTP requires longer to resolve remains a question to be addressed, but one may speculate that recurrent disease by itself defines more severe states of autoimmunity. In the future, larger cohorts may help to identify other factors that correlate with the time to resolution of autoimmunity.
As outlined previously, this retrospective observational study has several limitations, including that it comprised very heterogeneous treatment regimens. Another limitation was the fact that based on the published aTTP disease incidence in Germany of 2.1 per 1 000 000 per year, only ∼25% to 30% of cases treated for aTTP in Germany during the observation period received caplacizumab.19,20 There seems to be a certain bias regarding disease severity and the use of caplacizumab and rituximab.
In summary, the significance of ADAMTS13 activity measurements has gained much interest. Its immediate availability poses a logistical challenge but will lead to significant cost savings without jeopardizing the well-being of patients with aTTP. It seems reasonable to tailor a caplacizumab treatment regimen based on ADAMTS13 activities. Based on these findings, we estimate that ∼20% of patients require caplacizumab beyond day 30, but that the majority of patients can be treated with a shorter treatment course, resulting in significant cost savings. In addition, VWF activity measurements allow monitoring of caplacizumab pharmacodynamic parameters to further reduce treatment costs and side effects during this life-saving treatment.
Results presented in this article have not been published previously except in abstract form at the Kidney Week 2019 of the American Society of Nephrology (ASN) and the Congress of Nephrology 2019 of the Germany Society of Nephrology (DGfN).
All data requests should be submitted to the corresponding authors (Paul T. Brinkkoetter [e-mail: paul.brinkkoetter@uk-koeln.de] or Jan Menne [e-mail: menne.jan@mh-hannover.de or jan.menne@krh.de]).
Authorship
Contribution: P.T.B. and J.M. contributed to conceptualization; L.A.V., J.K., P.T.B., and J.M. contributed to the Methods; L.A.V. and H.C. performed statistical analyses and calculations; L.A.V., J.K., S.B., A.M., A.S., J. Gaedeke, M.T., W.J.J., F.Ö., W.M., S.M., M.G., F.B., T.H.W., H.F., M.H., M.B., J. Gerth, M. Bieringer, M. Bommer, S.Z., J.S., S.E., A. Gawlik, A. Gäckler, A.K., V.S., U.S., M.R., J.R., J.B., A.M., R.H, A.H., S.P., R.W., C.v.A., P.T.B., and J.M. performed investigations; L.A.V., J.K., L.K., P.T.B., and J.M. were responsible for writing, reviewing, and editing the manuscript; and P.T.B. and J.M. were responsible for study initiation and supervision.
Conflict-of-interest disclosure: P.T.B. reports grants from the German Research Foundation (BR2955/8) during the conduct of the study; and personal fees from Alexion, Astellas, Bayer, Sanofi Genzyme, Pfizer, and Vifor (speaker honoraria and advisory boards). L.A.V. reports grants from the Else-Kroener-Fresenius Stiftung (2015_A224); and speaker honoraria from Sanofi Genzyme. S.B. receives grant support from the German Research Foundation (BR4917/3). J.M. received personal fees from Alexion, Sanofi Genzyme, and Ablynx (speaker honoraria and advisory boards). S.A.P. received personal fees from Alexion, Sanofi Genzyme, and Ablynx (speaker honoraria and advisory boards). R.W. received personal fees from Alexion, Sanofi Genzyme, and Ablynx (speaker honoraria, advisory boards, educational materials, and review writing). W.J.J. received speaker honoraria from Alexion and Ablynx (advisory boards). W.M. received honoraria from Ablynx, Takeda, and Shire (speaker honoraria and advisory boards). M.T. reports research grants from the Sonnenfeld Stiftung, Charité3R, and Novartis; and personal fees from Baxter, Cytosorbents, Novartis, and Takeda (speaker honoraria and advisory boards). M.R. reports personal fees from Alexion, Diamed, Roche, and Sanofi Genzyme (speaker honoraria and travel support). A. Gäckler reports personal fees from Alexion and Ablynx (speaker honoraria and advisory boards), F.B. received honoraria from Amgen, Sanofi, Akcea, Hexal, MSD, AstraZeneca, Alexion, and Astellas (speaker honoraria and advisory boards). U.S. reports study fees, travel support, and consultancy fees from Alexion; and study fees and consultancy fees Ablynx. M. Bommer received honoraria from Ablynx, Alexion, Amgen, and Sanofi; and study fees from Ablynx and Amgen. C.v.A. reports personal fees from Sanofi Genzyme (advisory boards). The remaining authors declare no competing financial interests.
Correspondence: Paul T. Brinkkoetter, Department II of Internal Medicine and Center for Molecular Medicine Cologne (CMMC), University of Cologne, Kerpener Str 62, D-50937 Cologne, Germany; e-mail: paul.brinkkoetter@uk-koeln.de; or Jan Menne, Department of Nephrology and Hypertension, Medical School Hannover, Carl-Neuberg-Str 1, 30625 Hannover, Germany; e-mail: menne.jan@mh-hannover.de or jan.menne@krh.de.

