

Key Points
Apixaban may serve as a reasonable alternative compared with warfarin in patients with severe renal dysfunction.

Abstract
Apixaban in patients with impaired renal function is supported by limited data. Landmark clinical trials evaluating apixaban in patients with atrial fibrillation and/or acute venous thromboembolism excluded patients with creatinine clearance (CrCl) <25 mL/min. This multicenter, retrospective chart review was conducted to evaluate the safety and effectiveness of apixaban compared with warfarin in patients with CrCl <25 mL/min. Included patients were newly initiated on apixaban or warfarin for at least 45 days with a CrCl <25 mL/min. Patients were evaluated for thrombosis and bleeding outcomes 6 months following initiation of anticoagulation. The primary outcome was the time to first bleeding or thrombosis event. A total of 128 patients met inclusion criteria in the apixaban group and 733 patients in the warfarin group. Time to first bleeding or thrombosis event was significantly different between the apixaban and warfarin groups. Cox proportional hazards model was conducted to control for potential confounding factors for the primary outcome. After controlling for atrial fibrillation and coronary artery bypass grafting, risk of thrombotic and bleeding events was lower in the apixaban group (hazard ratio, 0.47; 95% confidence interval, 0.25-0.92). There was not a statistical difference between time to thrombosis (83 days vs 54 days, P = .648), rate of thrombosis (5.5% vs 10.3%, P = .08), time to bleeding (46 days vs 54 days, P = .886), or rate of bleeding (5.5% vs 10.9%, P = .06). The severity of bleeding and thrombotic events was not different between groups. Apixaban may serve as a reasonable alternative compared with warfarin in patients with severe renal dysfunction.
Introduction
Therapeutic anticoagulation options for patients with chronic kidney disease or end-stage renal disease (ESRD) are limited. Historically, warfarin was the gold standard in these patients because of a lack of data with alternative oral agents.1-5 Landmark studies comparing apixaban with warfarin in atrial fibrillation and acute venous thromboembolism (VTE) excluded individuals with creatinine clearance (CrCl) <25 mL/min.6-8 However, in 2014 the US Food and Drug Administration (FDA) approved apixaban for ESRD patients with atrial fibrillation based on limited pharmacokinetic data.9 There are no dose changes recommended in patients with ESRD who are being treated with apixaban for VTE.
The expansion of FDA approval was based on a study performed by Chang et al, which evaluated the pharmacokinetics and pharmacodynamics of single-dose apixaban 10 mg in 32 patients, 7 with severe renal dysfunction (CrCl <30 mL/min). Results revealed an increase in apixaban area under the curve (AUC) by 44%; however, no difference in anti-factor Xa activity was observed.10 In addition Wang et al evaluated 8 patients on hemodialysis (HD) and found an increase in AUC by 36% and no difference in anti-factor Xa activity. Only a small percentage (6.7%) of the apixaban dose was recovered in the dialysate, showing HD has limited impact on apixaban clearance.11 Although single-dose pharmacokinetic studies demonstrated a small increase in AUC, steady-state pharmacokinetic analysis has shown a larger increase. Mavrakanas et al analyzed apixaban at steady state in 7 HD patients. AUC increased by two- to 5.7-fold in patients on apixaban 5 mg twice daily compared with apixaban 2.5 mg twice daily.12 Theoretically, the increase in AUC could lead to an increased risk of bleeding.
At the time of our study design, there was a lack of clinical data to support the safety and effectiveness of apixaban use in patients with severe renal dysfunction. Recently, studies evaluating apixaban vs warfarin in patients with CrCl <25 mL/min have suggested apixaban may be a reasonable alternative to warfarin.13-21 The purpose of this study was to evaluate the safety and effectiveness of apixaban vs warfarin in patients with CrCl <25 mL/min.
Design and methods
This multicenter retrospective cohort study was conducted across 7 hospitals in southeastern Michigan between January 2013 and December 2015. Adult patients, age 18 to 89 years, were included if they were newly initiated on warfarin or apixaban and their CrCl was <25 mL/min. Patients were excluded if intended anticoagulation treatment was <45 days or if they were pregnant. Institutional review board approval was obtained at each respective site.
The primary outcome was time to first bleeding or thrombotic event in apixaban patients compared with warfarin patients. Bleeding was defined using the Thrombolysis in Myocardial Infarction bleeding criteria.22 Thrombotic event severity criteria were used to categorize acute coronary syndrome, stroke, and VTE events (Table 1). Patients were evaluated for outcomes within 6 months following initiation of anticoagulation. Secondary outcomes included time to first bleeding event, time to first thrombosis event, proportion of patients experiencing bleeding, proportion of patients experiencing thrombosis, severity and source of bleeding, and severity and source of thrombosis. A subgroup analysis was performed on the primary outcome to explore the effect of apixaban 2.5 mg twice daily vs 5 mg twice daily.
Thromboembolic event severity
| Severity | Criteria |
|---|---|
| Major | ACS: mortality, ICU requirement, 3-vessel disease |
| DVT/PE: mortality, ICU requirement, intubation requirement, tPA admin, EKOS | |
| Stroke: mortality, ICU requirement, causes severe disability and cannot carry out IADL | |
| Minor | ACS: not meeting “major” or “minimal” criteria, stenting, PTCA |
| DVT/PE: event causing hospitalization, but otherwise hemodynamically stable | |
| Stroke: causes slight disability but can carry out most or moderate IADL | |
| Minimal | ACS: symptomatic management only, 23-h observation, no prescription change |
| DVT/PE: symptomatic or discharged on anticoagulation without being admitted | |
| Stroke: no symptoms (NIHSS of ∼0-3) or no significant disability |
| Severity | Criteria |
|---|---|
| Major | ACS: mortality, ICU requirement, 3-vessel disease |
| DVT/PE: mortality, ICU requirement, intubation requirement, tPA admin, EKOS | |
| Stroke: mortality, ICU requirement, causes severe disability and cannot carry out IADL | |
| Minor | ACS: not meeting “major” or “minimal” criteria, stenting, PTCA |
| DVT/PE: event causing hospitalization, but otherwise hemodynamically stable | |
| Stroke: causes slight disability but can carry out most or moderate IADL | |
| Minimal | ACS: symptomatic management only, 23-h observation, no prescription change |
| DVT/PE: symptomatic or discharged on anticoagulation without being admitted | |
| Stroke: no symptoms (NIHSS of ∼0-3) or no significant disability |
ACS, acute coronary syndrome; DVT, deep vein thrombosis; EKOS, catheter-assisted thrombolysis; IADL, instrumental activities of daily living; ICU, intensive care unit; NIHSS, National Institutes of Health stroke scale; PE, pulmonary embolism; tPA, tissue plasminogen activator; PTCA, percutaneous transluminal coronary angioplasty.
Data were electronically extracted from electronic medical records and input to Microsoft Access (2016). Primary outcome data were manually collected. The Cockcroft-Gault equation was used to calculate CrCl using admission age, actual body weight (ABW) or adjusted body weight (AjBW), and discharge serum creatinine. In obese patients, defined as total body weight >130% of ideal body weight (IBW), an AjBW was used (AjBw = IBW + 0.4[ABW − IBW]). A CrCl <25 mL/min was defined as renal dysfunction. International Classification of Diseases (ICD)-9 and ICD-10 codes documented at the index hospitalization were used to determine the presence of comorbidities. After data were collected at each site, patient records were deidentified and combined for analysis. Each site conducted a manual chart review on 2% of the total sample to verify the accuracy of extracted data.
Descriptive data were expressed as mean ± the standard deviation, median (interquartile range), or frequencies and percentage. Univariable analysis was performed using Student t, Mann-Whitney U, or χ2 test for continuous, ordinal, and categorical data, respectively. Post hoc testing of χ2 test was performed if P < .05 by calculating adjusted residuals. Time to first bleeding or thrombotic event was assessed using the log-rank test or Cox proportional hazards model for univariable and multivariable analysis, respectively. Variables were initially considered for inclusion if there was a difference between the apixaban and the warfarin group and there was an association with time to first bleeding or thrombosis event (P < .1). All statistical analyses were performed using SPSS software, version 24. P < .05 was considered to be statistically significant.
Results
Data from 4 different health systems, encompassing 7 separate institutions were included in the study. Patients were included from the following health systems: Ascension St. John Hospital System (n = 197), Beaumont Hospital – Royal Oak (n = 161), Detroit Medical Center (n = 320), and Henry Ford Hospital (n = 183). A total of 128 patients met inclusion criteria in the apixaban group, and 733 patients were included in the warfarin group. Baseline characteristics are presented in Table 2. Patients in both groups were predominantly female (57.8% [apixaban] vs 52.4% [warfarin]). Patients in the apixaban group were older compared with the warfarin group (74 years vs 67 years, P < .01). Additionally, the apixaban group had a significantly higher rate of heart failure (53.1% vs 35.7%, P < .01), history of atrial fibrillation (63.3% vs 29.5%, P < .01), stent placement (17.2% vs 6%, P < .01), and hyperlipidemia (44.5% vs 29.7%, P < .01). In the warfarin group, patients had a higher rate of prior VTE (32.1% vs 14.4%, P < .01). All other baseline demographics and patient characteristics were similar between the 2 groups.
Baseline characteristics
| Apixaban (n = 128) | Warfarin (n = 733) | P | |
|---|---|---|---|
| Age, mean (±SD), y | 74 (±14) | 67 (±15) | <.01 |
| Female, n (%) | 74 (57.8) | 384 (52.4) | .256 |
| Comorbidities, n (%) | |||
| Heart failure | 68 (53.1) | 262 (35.7) | <.01 |
| Atrial fibrillation | 81 (63.3) | 216 (29.5) | <.01 |
| DVT/PE | 21 (14.4) | 235 (32.1) | <.01 |
| Hypertension | 57 (44.5) | 387 (52.8) | .086 |
| History of stroke | 16 (12.5) | 92 (12.6) | 1 |
| Myocardial infarction | 27 (21.1) | 167 (22.8) | .73 |
| History of bleeding | 8 (6.3) | 44 (6) | .84 |
| CABG | 13 (10.2) | 42 (4.7) | .08 |
| Diabetes | 44 (34.4) | 273 (37.2) | .55 |
| Hyperlipidemia | 57 (44.5) | 218 (29.7) | <.01 |
| Peripheral artery disease | 15 (11.7) | 58 (7.9) | .17 |
| History of smoking | 32 (25) | 120 (16.4) | .02 |
| History of falls | 5 (3.9) | 18 (2.5) | .37 |
| Hypercoagulable | 0 (0.0) | 9 (1.2) | .37 |
| Hemodialysis | 21 (16.4) | 118 (16.1) | .90 |
| Renal transplant | 0 (0) | 18 (2.5) | .09 |
| Liver disease | 13 (10.2) | 56 (7.6) | .38 |
| Laboratory values, median (IQR) | |||
| Study CrCl, mL/min | 18.7 (12.3,22.6) | 14.8 (10.1,19.5) | <.01 |
| Baseline INR | 1.2 (1.1,1.5) | 1.1 (1.1,1.2) | .03 |
| Baseline hemoglobin, g/dL | 10.2 (9.1,11.8) | 9.7 (8.5,11) | <.01 |
| Anticoagulation indication, n (%) | |||
| Atrial fibrillation/flutter | 71 (55.5) | 226 (30.8) | <.01 |
| History of atrial fibrillation | 26 (20.3) | 32 (4.4) | <.01 |
| Acute VTE | 20 (15.6) | 350 (47.7) | <.01 |
| Chronic VTE | 3 (2.3) | 7 (1) | .19 |
| Valve replacement | 0 (0) | 16 (2.2) | .09 |
| Cardiac thrombus | 2 (1.6) | 17 (2.3) | .55 |
| Other | 0 (0) | 40 (5.5) | .01 |
| Multiple | 6 (4.7) | 45 (6.1) | .48 |
| Concomitant agents, n (%) | |||
| Aspirin | 82 (64.1) | 473 (64.5) | .92 |
| Clopidogrel | 9 (7) | 86 (11.7) | .12 |
| Cilostazol | 7 (5.5) | 20 (2.7) | .10 |
| Ticagrelor | 1 (0.8) | 3 (0.4) | .48 |
| Apixaban dosing, n (%) | |||
| 2.5 mg twice daily | 73 (57) | ||
| 5 mg twice daily | 55 (43) | ||
| Incorrect dosing | 21 (16.4) | ||
| Apixaban (n = 128) | Warfarin (n = 733) | P | |
|---|---|---|---|
| Age, mean (±SD), y | 74 (±14) | 67 (±15) | <.01 |
| Female, n (%) | 74 (57.8) | 384 (52.4) | .256 |
| Comorbidities, n (%) | |||
| Heart failure | 68 (53.1) | 262 (35.7) | <.01 |
| Atrial fibrillation | 81 (63.3) | 216 (29.5) | <.01 |
| DVT/PE | 21 (14.4) | 235 (32.1) | <.01 |
| Hypertension | 57 (44.5) | 387 (52.8) | .086 |
| History of stroke | 16 (12.5) | 92 (12.6) | 1 |
| Myocardial infarction | 27 (21.1) | 167 (22.8) | .73 |
| History of bleeding | 8 (6.3) | 44 (6) | .84 |
| CABG | 13 (10.2) | 42 (4.7) | .08 |
| Diabetes | 44 (34.4) | 273 (37.2) | .55 |
| Hyperlipidemia | 57 (44.5) | 218 (29.7) | <.01 |
| Peripheral artery disease | 15 (11.7) | 58 (7.9) | .17 |
| History of smoking | 32 (25) | 120 (16.4) | .02 |
| History of falls | 5 (3.9) | 18 (2.5) | .37 |
| Hypercoagulable | 0 (0.0) | 9 (1.2) | .37 |
| Hemodialysis | 21 (16.4) | 118 (16.1) | .90 |
| Renal transplant | 0 (0) | 18 (2.5) | .09 |
| Liver disease | 13 (10.2) | 56 (7.6) | .38 |
| Laboratory values, median (IQR) | |||
| Study CrCl, mL/min | 18.7 (12.3,22.6) | 14.8 (10.1,19.5) | <.01 |
| Baseline INR | 1.2 (1.1,1.5) | 1.1 (1.1,1.2) | .03 |
| Baseline hemoglobin, g/dL | 10.2 (9.1,11.8) | 9.7 (8.5,11) | <.01 |
| Anticoagulation indication, n (%) | |||
| Atrial fibrillation/flutter | 71 (55.5) | 226 (30.8) | <.01 |
| History of atrial fibrillation | 26 (20.3) | 32 (4.4) | <.01 |
| Acute VTE | 20 (15.6) | 350 (47.7) | <.01 |
| Chronic VTE | 3 (2.3) | 7 (1) | .19 |
| Valve replacement | 0 (0) | 16 (2.2) | .09 |
| Cardiac thrombus | 2 (1.6) | 17 (2.3) | .55 |
| Other | 0 (0) | 40 (5.5) | .01 |
| Multiple | 6 (4.7) | 45 (6.1) | .48 |
| Concomitant agents, n (%) | |||
| Aspirin | 82 (64.1) | 473 (64.5) | .92 |
| Clopidogrel | 9 (7) | 86 (11.7) | .12 |
| Cilostazol | 7 (5.5) | 20 (2.7) | .10 |
| Ticagrelor | 1 (0.8) | 3 (0.4) | .48 |
| Apixaban dosing, n (%) | |||
| 2.5 mg twice daily | 73 (57) | ||
| 5 mg twice daily | 55 (43) | ||
| Incorrect dosing | 21 (16.4) | ||
aPTT, activated partial thromboplastin time; CABG, coronary artery bypass graft; INR, international normalized ratio; TIA, transient ischemic stroke.
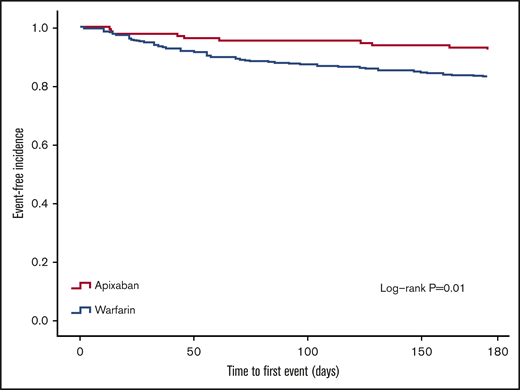
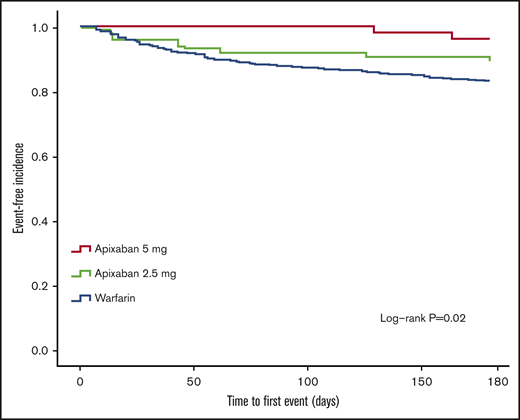
Time to first bleeding or thrombotic event was significantly different between the apixaban and warfarin groups (Figure 1). Cox proportional hazards model was conducted to control for potential confounding factors for the primary outcome (Table 3). After controlling for atrial fibrillation and coronary artery bypass grafting, risk of thrombotic or bleeding events was less in the apixaban group (hazard ratio [HR], 0.47; 95% confidence interval [CI], 0.25-0.92). A post hoc analysis controlling for all differences in baseline characteristics (P < .05, including age and history of atrial fibrillation, heart failure, VTE, hyperlipidemia, and smoking) found similar results (0.47, 95% CI, 0.24-0.91). There was not a statistical difference between groups for time to thrombosis (83 days vs 54 days, P = .648), rate of thrombosis (5.5% vs 10.3%, P = .08), time to bleeding (46 days vs 54 days, P = .886), or rate of bleeding (5.5% vs 10.9%, P = .06). The severity of events, both bleeding and thrombotic, was not different between groups (Table 4). Mortality was not different between warfarin and apixaban (14.9% vs 11.8% respectively, P = .72). A subgroup analysis was conducted to identify differences between apixaban 5 mg twice daily, apixaban 2.5 mg twice daily, and warfarin. Patients receiving apixaban 5 mg twice per day had a longer time to first event (P = .02; Figure 2), which was driven by a lower rate of bleeding (0% for 5 mg, 9.5% for 2.5 mg, and 10.5% for warfarin, P = .04) with no difference in thrombosis (P = .374).
Secondary outcomes
| Thromboembolic outcomes | Apixaban (n = 28) | Warfarin (n = 733) | P |
|---|---|---|---|
| Total events, % | 5.5 | 10.3 | .08 |
| NSTEMI, n (%) | 5 (3.9) | 21 (2.9) | .572 |
| STEMI, n (%) | 0 (0) | 6 (0.8) | .6 |
| CVA, n (%) | 0 (0) | 10 (1.4) | .374 |
| DVT, n (%) | 1 (0.8) | 23 (3.1) | .238 |
| PE, n (%) | 0 (0) | 4 (0.5) | 1.0 |
| Cardiac thrombus, n (%) | 1 (0.8) | 12 (1.6) | .704 |
| Clot severity, n (%) | |||
| Major | 1 (0.8) | 9 (1.2) | .634 |
| Minor | 5 (3.9) | 43 (5.9) | |
| Minimal | 0 (0) | 8 (1.1) | |
| Bleeding outcomes, % | 5.5 | 10.9 | |
| Brain, n (%) | 0 (0) | 5 (0.7) | .06 |
| GI bleed, n (%) | 6 (4.7) | 67 (9.1) | |
| Hematuria, n (%) | 1 (0.8) | 6 (0.8) | |
| Other, n (%) | 0 (0) | 2 (0.3) | |
| Bleed severity, n (%) | |||
| Major | 1 (0.8) | 12 (1.6) | .474 |
| Minor | 5 (3.9) | 61 (8.3) | |
| Minimal | 1 (0.8) | 3 (0.4) | |
| Thromboembolic outcomes | Apixaban (n = 28) | Warfarin (n = 733) | P |
|---|---|---|---|
| Total events, % | 5.5 | 10.3 | .08 |
| NSTEMI, n (%) | 5 (3.9) | 21 (2.9) | .572 |
| STEMI, n (%) | 0 (0) | 6 (0.8) | .6 |
| CVA, n (%) | 0 (0) | 10 (1.4) | .374 |
| DVT, n (%) | 1 (0.8) | 23 (3.1) | .238 |
| PE, n (%) | 0 (0) | 4 (0.5) | 1.0 |
| Cardiac thrombus, n (%) | 1 (0.8) | 12 (1.6) | .704 |
| Clot severity, n (%) | |||
| Major | 1 (0.8) | 9 (1.2) | .634 |
| Minor | 5 (3.9) | 43 (5.9) | |
| Minimal | 0 (0) | 8 (1.1) | |
| Bleeding outcomes, % | 5.5 | 10.9 | |
| Brain, n (%) | 0 (0) | 5 (0.7) | .06 |
| GI bleed, n (%) | 6 (4.7) | 67 (9.1) | |
| Hematuria, n (%) | 1 (0.8) | 6 (0.8) | |
| Other, n (%) | 0 (0) | 2 (0.3) | |
| Bleed severity, n (%) | |||
| Major | 1 (0.8) | 12 (1.6) | .474 |
| Minor | 5 (3.9) | 61 (8.3) | |
| Minimal | 1 (0.8) | 3 (0.4) | |
CVA, cerebrovascular accident; GI, gastrointestinal; NSTEMI, non-ST-elevation myocardial infarction; STEMI, ST-elevation myocardial infarction.
Cox proportional hazard model evaluating the association between apixaban and time to bleeding or thrombosis
| Variable | Hazard ratio (95% CI) | P |
|---|---|---|
| Apixaban (vs warfarin) | 0.47 (0.25-0.92) | .03 |
| Atrial fibrillation | 0.66 (0.44-0.98) | .04 |
| CABG | 2.58 (1.51-4.39) | <.01 |
| Variable | Hazard ratio (95% CI) | P |
|---|---|---|
| Apixaban (vs warfarin) | 0.47 (0.25-0.92) | .03 |
| Atrial fibrillation | 0.66 (0.44-0.98) | .04 |
| CABG | 2.58 (1.51-4.39) | <.01 |
Discussion
The results from this multicenter cohort study suggest apixaban may be a reasonable option for patients with severe renal dysfunction despite the known increase in apixaban exposure.11,12 These results add to the growing body of evidence of real-world data that apixaban is a reasonable option for patients with severe renal dysfunction. Apixaban was associated with a decreased composite risk of bleeding and thrombosis compared with warfarin. Furthermore, the apixaban 5 mg twice per day dose was not associated with increased risk of bleeding, which supports the package insert dosing in this population. In previous studies, patients with renal dysfunction receiving apixaban have been underdosed based on the package insert recommendations.18,19,21 23 These findings should decrease uneasiness surrounding FDA recommended dosing. Our study noted differences in prescribing practices for apixaban and warfarin in ESRD patients across the multiple health care systems included. Apixaban tended to be prescribed in older patients with a history of atrial fibrillation rather than those with DVT/PE.
The results of this study are in concordance with recently published retrospective studies evaluating the safety and effectiveness of apixaban compared with warfarin in patients in severe renal dysfunction.17-19,21 A retrospective study conducted by Schafer et al included a total of 604 patients with chronic kidney disease stage 4, stage 5, and dialysis receiving apixaban or warfarin for the treatment of atrial fibrillation or VTE.19 Similar rates of major bleeding between apixaban and warfarin were observed at 3 and 6 months, without any difference in rates of ischemic stroke or thromboembolism. A higher incidence of major bleeding with warfarin was observed in patients who continued therapy for 6 and 12 months. Of note, the study reported approximately one-third of patients in the apixaban group received the incorrect dosage. Additionally, Siontis et al performed a study evaluating apixaban patients on HD and found lower rates of major bleeding compared with warfarin. The study also found that apixaban 5 mg twice daily, but not apixaban 2.5 mg twice daily, was associated with lower risk of thromboembolic events and mortality compared with warfarin. The data used in this study were obtained from an insurance claims database and information on body weight could not be obtained; therefore, appropriateness of dosing could not be assessed.20
One strength of this retrospective review is its use of data from multiple institutions. Although the exact patient data could not be shared because of Health Insurance Portability and Accountability Act and institutional review board constraints, patients could be deidentified systematically to allow multiple institutions to confirm patients and outcomes. For instance, a participant could be discharged from Henry Ford Hospital on apixaban but admitted with a major bleeding episode at Beaumont Hospital and still be recorded as having an event as long as both institutions assigned the same study code to the patient. This allowed the study team to observe additional events between hospital systems that would not have been reported otherwise because the patient would have simply been “lost to follow-up” and assumed alive and well. Given that these institutions represent well in excess of 50% of metro Detroit-area emergency room visits, it is very likely that patients discharged from any institution would arrive at any 1 of the study sites rather than a nonstudy site.
Our study has several limitations. First, patients on HD whose CrCl was calculated to be >25 mL/min were not included in the study because of exclusion criteria. However, few HD patients would fall into this subpopulation of patients. Second, adherence to study drug and other prescription or nonprescription medications could not be measured. This could potentially increase the risk of bleeding or thrombosis. Third, each site relied heavily on ICD-9 and ICD-10 codes for baseline characteristics and outcomes. This minimized the need for manual chart review and allowed for a larger sample of patients but could have decreased the accuracy of the data. Quality assessment was performed by manual chart review on all outcome data to ensure accurate information was being obtained. Last, despite a large sample size, many of our secondary outcomes were underpowered to detect a difference.
Overall, we observed a decrease in composite risk of bleeding or thrombosis in patients receiving apixaban vs warfarin. Apixaban may serve as a reasonable alternative compared with warfarin in patients with severe renal dysfunction. Further evaluation, in a prospective manner, of the use of apixaban in patients with a severe renal dysfunction, especially those on hemodialysis, is needed to definitively determine the role of apixaban in this patient population.
For original data, please contact Claudia Hanni (claudiahanni@gmail.com).
Acknowledgments
The study group thanks Elizabeth Crish, Lorraine Tarpley, Ellen Muniga, Jona Lekura, and Elizabeth Wilpula for their involvement and assistance during various stages of the study.
Authorship
Contribution: All authors participated in designing and performing research, analyzing data, and writing the paper.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Claudia Hanni, Anticoagulation/Internal Medicine, Beaumont Hospital–Royal Oak, 3601 West 13 Mile Rd, Royal Oak, MI 48073; e-mail: claudiahanni@gmail.com.

