

Key Points
Short-term data suggest that stage I/II NLPHL can be treated with ISRT without a negative impact on disease-free survival.

Abstract
Radiation fields for limited-stage nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) have shrunk over time; involved-site radiation therapy (ISRT) has replaced extended-field radiation therapy (EFRT) and involved-field radiation therapy (IFRT), but this has not been validated. The role of systemic therapy is unclear. We reviewed 71 stage I/II NLPHL patients and assessed progression-free survival (PFS), overall survival (OS), locoregional disease-free survival, and distant disease-free survival (DDFS). Median patient age was 39 years, and 61% had stage II disease. Thirty-six (51%) received radiation therapy (RT) only, 6 (8%) received systemic therapy only, and 29 (41%) received both. More patients receiving combined therapy had B symptoms (P = .035) and stage II disease (P = .001). In the RT-only group, 9 (25%) received EFRT, 13 (36%) received IFRT, and 14 (39%) received ISRT; in the combined-modality group, 3 (10%) received EFRT, 7 (24%) received IFRT, and 19 (66%) received ISRT. After a median follow-up of 6.2 years, 15 patients relapsed (13 distant, 2 locoregional). Five-year PFS and OS rates were 86% and 96% and did not differ by treatment. In the RT-only group, follow-up was shorter in the ISRT cohort (2.6 years vs 17.9 years [EFRT] and 8.5 years [IFRT], P < .01), but 5-year PFS did not differ by field size (P = .20). Locoregional control rates were 100% for the RT-only and combined groups, and corresponding 5-year DDFS rates were 93% and 95% (P = .95). Eight patients (11%) experienced a second malignancy (1 within RT field). Six patients died (1 from lymphoma). Use of limited ISRT fields does not appear to increase the risk of locoregional relapse, even when RT is given as single-modality therapy.
Introduction
Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) is a rare and clinically indolent type of Hodgkin lymphoma (HL) that is characterized by distinctive CD20+ lymphocyte-predominant cells in a background of small lymphocytes and histiocytes. The optimal treatment strategy for patients with NLPHL is controversial, because this disease is often not life-threatening, and therapies for relapsed disease are effective. Roughly two thirds of patients present with limited-stage disease and, in contrast to patients with classical HL, late relapses are frequent.1 Treatment options include observation, systemic therapy, definitive radiation therapy (RT), and combined-modality therapy (CMT). Immunotherapy with CD20-targeted agents also has been explored for initial treatment and relapsed disease.2-6
For stage I-II classical HL, CMT and systemic therapy alone have been shown, in randomized studies, to produce excellent outcomes, with CMT offering improvements in disease control.7-12 Given the rarity of NLPHL, prospective studies are difficult, and treatment recommendations vary. Options include RT alone or CMT; however, whether the addition of systemic therapy improves outcomes is unclear, because the data are limited and conflicting.13-16 Historically, RT alone produced excellent disease control, but the use of high radiation doses and large extended fields led to correspondingly high rates of late treatment–related morbidity and mortality. Use of smaller RT fields coupled with lower RT doses would be expected to result in reduced long-term toxicity, but whether this compromises disease control is unclear, especially when RT alone is used to treat NLPHL. Here, we sought to evaluate the effect of systemic therapy on disease outcomes and determine the effect of RT field size on treatment efficacy, with the goal of determining whether the use of limited involved-site fields influenced disease control in patients with early-stage NLPHL treated over a 30-year period at a single institution.
Methods
With the approval of the MD Anderson Cancer Center Institutional Review Board, we searched our institutional lymphoma database for adult patients (≥18 years) treated for stage I/II NLPHL from 1987 through 2017. The initial screen yielded 85 patients. Fourteen patients were excluded, 9 for lack of follow-up after completing therapy, 3 for having transformed disease at diagnosis, and 2 who were observed and who did not receive initial therapy. Twenty-six patients included in the current study were also part of a previous analysis.5 The pathologic specimens were reviewed by hematopathologists using World Health Organization criteria.17 Tumor growth pattern was classified histologically as typical (patterns A and B) or variant (patterns C-F), according to established criteria.18,19 Clinical characteristics at the time of diagnosis were recorded. Disease stage was assigned according to the Ann Arbor system.20 All patients underwent baseline staging assessment with computed tomography (CT). Patients diagnosed in 2002 or later were also assessed with baseline positron emission tomography (PET)–CT. The maximum nodal diameter in the axial plane was determined. For patients who had PET-CT imaging, the maximum standardized uptake value (SUV) was recorded. Our MD Anderson Cancer Center Institutional Review Board approved this retrospective study and waived the informed consent requirement in accordance with the Declaration of Helsinki.
Systemic therapy
For patients given systemic therapy, the most common regimens were immunochemotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) or doxorubicin, bleomycin, vinblastine, and dacarbazine without or with rituximab (ABVD or R-ABVD, respectively). When rituximab alone was used, it was given weekly for a total of 4 doses.
Radiation therapy
Details of RT were extracted from the medical record. Patients who received RT with subtotal nodal, mantle, or total abdominopelvic fields were classified as having received extended-field radiation therapy (EFRT). Those who were treated with fields that encompassed the involved nodal area, as well as adjacent radiographically uninvolved nodal tissue, were classified as having had involved-field radiation therapy (IFRT), in accordance with guidelines published in 2002.21 Treatment to only the initially involved nodal regions, with a margin to account for differences in treatment position between the diagnostic CT images and RT treatment position, were considered involved-site radiation therapy (ISRT), according to guidelines from the International Lymphoma Radiation Oncology Group.22 The IFRT and ISRT treatment fields for 2 patients in this study are illustrated in Figure 1. The RT technique was traditional 3-dimensional conformal or intensity-modulated RT. The RT prescription dose delivered was recorded.

Treatment of stage IA NLPHL of the right neck with IFRT vs ISRT. Diagnostic PET-CT scout (A), coronal (B), and axial (D) images of a patient with fluorodeoxyglucose-avid stage IA NLPHL of the right neck treated with IFRT. Coronal (C) and axial (E) CT images from the 3-dimensional radiation treatment plan illustrate the gross disease (contoured in red) and the extended clinical treatment volume (contoured in yellow). Diagnostic PET-CT scout (F), coronal (G), and axial (I) images of a second patient with stage IA NLPHL of the right neck treated with ISRT. Coronal (H) and axial (J) images from the RT plan illustrate the gross tumor volume (contoured in red) and the more limited clinical tumor volume (contoured in yellow).
Treatment of stage IA NLPHL of the right neck with IFRT vs ISRT. Diagnostic PET-CT scout (A), coronal (B), and axial (D) images of a patient with fluorodeoxyglucose-avid stage IA NLPHL of the right neck treated with IFRT. Coronal (C) and axial (E) CT images from the 3-dimensional radiation treatment plan illustrate the gross disease (contoured in red) and the extended clinical treatment volume (contoured in yellow). Diagnostic PET-CT scout (F), coronal (G), and axial (I) images of a second patient with stage IA NLPHL of the right neck treated with ISRT. Coronal (H) and axial (J) images from the RT plan illustrate the gross tumor volume (contoured in red) and the more limited clinical tumor volume (contoured in yellow).
Response assessment
Response to therapy was determined after primary therapy but varied according to the time of diagnosis and therapy. For patients treated before the advent of PET-CT, treatment response was based on CT imaging per the 1999 International Working Group criteria.23 For patients who received PET-CT after therapy, response was recorded according to the International Working Group criteria that incorporated functional imaging.20
Study end points and statistical methods
Progression-free survival (PFS) and overall survival (OS) were calculated from the date of diagnosis to disease relapse, progression, or death from any cause (PFS) or death from any cause (OS). Locoregional disease-free survival (LDFS) was calculated from the date of diagnosis to the date of relapse or progression in the initially involved nodal region or the immediately adjacent Ann Arbor nodal region. Distant disease-free survival (DDFS) was calculated from the date of diagnosis to the date of disease relapse in an initially uninvolved Ann Arbor nodal region. For PFS, LDFS, and DDFS, the diagnosis of diffuse large B-cell lymphoma (DLBCL) was considered an event; however, a non-NLPHL/DLBCL second malignancy diagnosis was not. For LDFS and DDFS, patients were censored at the time of death or last follow-up. PFS and OS were censored at the time of last follow-up examination or patient contact. Survival times were estimated by using the Kaplan-Meier method, and differences between treatment groups were compared using log-rank tests.24 Survival times were censored at the time of last follow-up examination or patient contact. Potential associations between clinical and treatment factors and PFS and OS were assessed with a Cox proportional hazards model. Median follow-up times and 95% confidence intervals (CIs) were calculated by using the reverse Kaplan-Meier method.25 Median time to relapse was calculated among eligible patients. For categorical variables, Fisher’s exact tests were used to assess differences between the RT-only and combined-modality groups. To compare continuous variables, Student t tests were used. SPSS (version 24; IBM Analytics, Armonk, NY) and GraphPad Prism (version 7.01; GraphPad Software, La Jolla, CA) were used for all statistical analyses, and P < .05 was considered to indicate significant differences.
Results
We identified a total of 71 adult patients with confirmed NLPHL who had stage I or II disease at diagnosis (Table 1). The median patient age was 39 years, 53 (75%) patients were male, 56 (79%) presented with supradiaphragmatic disease, and 43 (61%) had stage II disease; 23 (32%) patients had a variant histologic pattern in the diagnostic biopsy specimen. Only 8 (11%) patients were treated before the year 2000. PET-CT imaging was used at diagnosis for 60 (85%) patients. In these patients, the maximum SUV was available for 44 patients, and the median value was 10.2 (range, 2.5-27.8). Univariate analysis revealed inferior PFS among patients who did not undergo PET-CT for initial staging (P = .016) and a nonsignificant trend toward inferior PFS for men (P = .080) (Table 2). Stage II disease at diagnosis was not associated with inferior PFS (P = .665) or OS (P = .425); indeed, no baseline clinical or disease characteristics were associated with OS on univariate analysis (Table 2).
Patient and disease characteristics
| Characteristic | All patients (N = 71) | RT only (n = 36) | Combined therapy (n = 29) | RT-only vs combined therapy, P | Systemic therapy only (n = 6) |
|---|---|---|---|---|---|
| Age | |||||
| Median (range), y | 39 (18-73) | 38 (18-69) | 40 (22-73) | 49 (31-68) | |
| ≥45 y | 30 (42) | 15 (42) | 11 (38) | .803 | 4 (67) |
| Male | 53 (75) | 26 (72) | 23 (79) | .573 | 4 (67) |
| Disease stage | |||||
| I | 28 (39) | 22 (61) | 6 (21) | .001 | 0 |
| II | 43 (61) | 14 (39) | 23 (79) | 6 (100) | |
| Disease location | |||||
| Above diaphragm | 56 (79) | 32 (89) | 21 (72) | .114 | 3 (50) |
| Below diaphragm | 15 (21) | 4 (11) | 8 (28) | 3 (50) | |
| Mediastinal involvement | 3 (4) | 2 (6) | 1 (3) | 1.00 | 0 |
| ECOG PS | |||||
| 0 | 64 (90) | 33 (92) | 27 (93) | 1.00 | 4 (67) |
| 1 | 7 (10) | 3 (8) | 2 (7) | 2 (33) | |
| B symptoms | 5 (7) | 0 | 4 (14) | .035 | 1 (17) |
| Extranodal disease | 4 (7) | 1 (3) | 3 (10) | .316 | 0 |
| Histologic pattern | |||||
| Typical | 48 (68) | 28 (78) | 17 (59) | .113 | 3 (50) |
| Variant | 23 (32) | 8 (22) | 12 (41) | 3 (50) | |
| PET-CT imaging | 60 (85) | 29 (81) | 25 (86) | .742 | 6 (100) |
| Tumor size* | |||||
| Median (range), cm | 3.0 (1.2-8.5) | 3.0 (1.4-6.9) | 3.3 (1.2-8.5) | 2.8 (1.2-3.0) | |
| ≥5 cm | 8 (11) | 3 (8) | 5 (18) | .282 | 0 |
| Characteristic | All patients (N = 71) | RT only (n = 36) | Combined therapy (n = 29) | RT-only vs combined therapy, P | Systemic therapy only (n = 6) |
|---|---|---|---|---|---|
| Age | |||||
| Median (range), y | 39 (18-73) | 38 (18-69) | 40 (22-73) | 49 (31-68) | |
| ≥45 y | 30 (42) | 15 (42) | 11 (38) | .803 | 4 (67) |
| Male | 53 (75) | 26 (72) | 23 (79) | .573 | 4 (67) |
| Disease stage | |||||
| I | 28 (39) | 22 (61) | 6 (21) | .001 | 0 |
| II | 43 (61) | 14 (39) | 23 (79) | 6 (100) | |
| Disease location | |||||
| Above diaphragm | 56 (79) | 32 (89) | 21 (72) | .114 | 3 (50) |
| Below diaphragm | 15 (21) | 4 (11) | 8 (28) | 3 (50) | |
| Mediastinal involvement | 3 (4) | 2 (6) | 1 (3) | 1.00 | 0 |
| ECOG PS | |||||
| 0 | 64 (90) | 33 (92) | 27 (93) | 1.00 | 4 (67) |
| 1 | 7 (10) | 3 (8) | 2 (7) | 2 (33) | |
| B symptoms | 5 (7) | 0 | 4 (14) | .035 | 1 (17) |
| Extranodal disease | 4 (7) | 1 (3) | 3 (10) | .316 | 0 |
| Histologic pattern | |||||
| Typical | 48 (68) | 28 (78) | 17 (59) | .113 | 3 (50) |
| Variant | 23 (32) | 8 (22) | 12 (41) | 3 (50) | |
| PET-CT imaging | 60 (85) | 29 (81) | 25 (86) | .742 | 6 (100) |
| Tumor size* | |||||
| Median (range), cm | 3.0 (1.2-8.5) | 3.0 (1.4-6.9) | 3.3 (1.2-8.5) | 2.8 (1.2-3.0) | |
| ≥5 cm | 8 (11) | 3 (8) | 5 (18) | .282 | 0 |
Unless otherwise noted, all data are n (%).
ECOG PS, Eastern Cooperative Oncology Group Performance Status score.
Tumor size was unavailable for 1 patient.
Univariate analysis
| Characteristic | PFS | OS | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Age | 1.01 (0.98-1.04) | .425 | 1.05 (0.99-1.11) | .107 |
| Male | 3.73 (0.86-16.30) | .080 | 1.65 (0.19-14.20) | .648 |
| Stage II | 1.26 (0.45-3.53) | .665 | 2.4 (0.28-20.65) | .425 |
| ECOG PS 1 | 1.04 (0.30-3.62) | .951 | 0.04 (0.00-265.72) | .461 |
| Supradiaphragmatic disease | 3.49 (0.80-15.24) | .097 | 31.38 (0.01-85 218.00) | .393 |
| B symptoms | 0.63 (0.08-4.80) | .630 | 0.05 (0.00-82 523.70) | .673 |
| Extranodal disease | 0.64 (0.08-4.90) | .670 | 2.79 (0.32-24.07) | .351 |
| Variant histologic pattern | 0.65 (0.24-1.82) | .417 | 0.39 (0.05-3.33) | .39 |
| PET-CT imaging not performed | 3.16 (1.24-8.04) | .016 | 4.38 (0.74-25.88) | .104 |
| Tumor size ≥5 cm | 0.95 (0.27-3.34) | .931 | 0.89 (0.10-7.65) | .913 |
| Era of therapy | ||||
| Before 2000* | ||||
| 2000-2010 | 0.55 (0.20-1.50) | .240 | 0.38 (0.08-1.97) | .251 |
| 2011-2017 | 0.24 (0.03-2.22) | .210 | <0.01 (0.00-1.6 × 10172) | .957 |
| Characteristic | PFS | OS | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Age | 1.01 (0.98-1.04) | .425 | 1.05 (0.99-1.11) | .107 |
| Male | 3.73 (0.86-16.30) | .080 | 1.65 (0.19-14.20) | .648 |
| Stage II | 1.26 (0.45-3.53) | .665 | 2.4 (0.28-20.65) | .425 |
| ECOG PS 1 | 1.04 (0.30-3.62) | .951 | 0.04 (0.00-265.72) | .461 |
| Supradiaphragmatic disease | 3.49 (0.80-15.24) | .097 | 31.38 (0.01-85 218.00) | .393 |
| B symptoms | 0.63 (0.08-4.80) | .630 | 0.05 (0.00-82 523.70) | .673 |
| Extranodal disease | 0.64 (0.08-4.90) | .670 | 2.79 (0.32-24.07) | .351 |
| Variant histologic pattern | 0.65 (0.24-1.82) | .417 | 0.39 (0.05-3.33) | .39 |
| PET-CT imaging not performed | 3.16 (1.24-8.04) | .016 | 4.38 (0.74-25.88) | .104 |
| Tumor size ≥5 cm | 0.95 (0.27-3.34) | .931 | 0.89 (0.10-7.65) | .913 |
| Era of therapy | ||||
| Before 2000* | ||||
| 2000-2010 | 0.55 (0.20-1.50) | .240 | 0.38 (0.08-1.97) | .251 |
| 2011-2017 | 0.24 (0.03-2.22) | .210 | <0.01 (0.00-1.6 × 10172) | .957 |
HR, hazard ratio.
The reference category is treatment before 2000.
The initial treatment strategy was RT only in 36 (51%) patients, CMT in 29 (41%) patients, and systemic therapy in 6 (9%) patients. All patients had a complete response to therapy. Compared with the RT-only group, the CMT group more often had stage II disease (P = .001) and B symptoms (P = .035; Table 1). Treatment details are listed in Table 3. Among patients who received CMT, R-CHOP was given before consolidative RT in 19 (66%) patients, whereas R-ABVD was given before consolidative RT in 4 (14%) patients and weekly rituximab was given before RT in 3 (10%) patients. The median number of chemotherapy cycles in the CMT group was 3 (range, 2-6). In the subgroup of patients who only received systemic therapy, 3 received R-CHOP, 2 received weekly rituximab, and 1 received R-ABVD, with a median of 6 cycles (range, 4-6). All patients who received systemic therapy only had a complete response to treatment. Among the 36 patients who received RT only, 9 (25%) received EFRT, 13 (36%) received IFRT, and 14 (39%) received ISRT. The median radiation dose in the RT-only group was 36 Gy (range, 30-40), with 72% of patients receiving >30.6 Gy. In the combined-therapy group, the median dose was 30.6 Gy (range, 21.6-40), with 21% of patients receiving >30.6 Gy; 3 patients (10%) had EFRT, 7 (24%) had IFRT, and 19 (66%) had ISRT.
Treatment and outcome characteristics
| Characteristic | All patients (N = 71) | RT only (n = 36) | Combined therapy (n = 29) | RT-only vs combined therapy, P | Systemic therapy (n = 6) |
|---|---|---|---|---|---|
| Treatment | |||||
| Systemic only | 6 (9) | ||||
| Radiation only | 36 (51) | ||||
| Combined | 29 (41) | ||||
| Treatment era | |||||
| Before 2000 | 8 (11) | 6 (17) | 2 (7) | .444 | 0 |
| 2000–2010 | 30 (42) | 14 (39) | 11 (38) | 5 (83) | |
| 2011–2017 | 33 (47) | 16 (44) | 16 (55) | 1 (17) | |
| Systemic therapy (n = 35) | |||||
| R-ABVD | 5 (7) | 4 (14) | 1 (17) | ||
| R-CHOP | 22 (31) | 19 (66) | 3 (50) | ||
| Rituximab | 5 (7) | 3 (10) | 2 (33) | ||
| Other | 3 (4) | 3 (10) | |||
| RT (n = 65) | |||||
| EFRT | 12 (17) | 9 (25) | 3 (10) | .088 | |
| IFRT | 20 (28) | 13 (36) | 7 (24) | ||
| ISRT | 33 (47) | 14 (39) | 19 (66) | ||
| RT (n = 65) | |||||
| 3-Dimensional | 39 (60) | 27 (75) | 12 (41) | .010 | |
| Intensity-modulated RT | 26 (40) | 9 (25) | 17 (59) | ||
| Radiation dose (n = 65) | |||||
| Median (range), Gy | 30.6 (21.6-40.0) | 36 (30-40) | 30.6 (21.6-40) | ||
| >30.6 Gy | 32 (49) | 26 (72) | 6 (21) | <.001 | |
| ≤30.6 Gy | 33 (51) | 10 (28) | 23 (79) | ||
| Death | |||||
| Yes | 6 (8) | 3 (8) | 2 (7) | 1 (17) | |
| No | 65 (92) | 33 (92) | 27 (93) | 5 (83) | |
| Relapse or progression | |||||
| Yes | 15 (21) | 8 (22) | 5 (17) | 2 (33) | |
| No | 56 (79) | 28 (78) | 24 (83) | 4 (67) | |
| Local relapse | |||||
| Yes | 2 (3) | 0 | 0 | 2 (33) | |
| No | 69 (97) | 36 (100) | 29 (100) | 4 (67) | |
| Distant relapse | |||||
| Yes | 13 (18) | 8 (22) | 5 (17) | 0 | |
| No | 58 (82) | 28 (78) | 24 (83) | 6 (100) | |
| Transformation | |||||
| Yes | 2 (3) | 1 (3) | 1 (3) | .876 | 0 |
| No | 69 (97) | 35 (97) | 28 (97) | ||
| Second malignancy | |||||
| Yes | 8 (11) | 3 (8) | 5 (17) | .277 | 0 |
| No | 63 (89) | 33 (92) | 24 (83) | 6 (100) | |
| Median follow-up (95% CI), y* | 6.1 (5.0-7.2) | 6.1 (3.3-8.9) | 4.4 (0.42–8.4) | .174 | 7.5 (4.0-11.0) |
| Characteristic | All patients (N = 71) | RT only (n = 36) | Combined therapy (n = 29) | RT-only vs combined therapy, P | Systemic therapy (n = 6) |
|---|---|---|---|---|---|
| Treatment | |||||
| Systemic only | 6 (9) | ||||
| Radiation only | 36 (51) | ||||
| Combined | 29 (41) | ||||
| Treatment era | |||||
| Before 2000 | 8 (11) | 6 (17) | 2 (7) | .444 | 0 |
| 2000–2010 | 30 (42) | 14 (39) | 11 (38) | 5 (83) | |
| 2011–2017 | 33 (47) | 16 (44) | 16 (55) | 1 (17) | |
| Systemic therapy (n = 35) | |||||
| R-ABVD | 5 (7) | 4 (14) | 1 (17) | ||
| R-CHOP | 22 (31) | 19 (66) | 3 (50) | ||
| Rituximab | 5 (7) | 3 (10) | 2 (33) | ||
| Other | 3 (4) | 3 (10) | |||
| RT (n = 65) | |||||
| EFRT | 12 (17) | 9 (25) | 3 (10) | .088 | |
| IFRT | 20 (28) | 13 (36) | 7 (24) | ||
| ISRT | 33 (47) | 14 (39) | 19 (66) | ||
| RT (n = 65) | |||||
| 3-Dimensional | 39 (60) | 27 (75) | 12 (41) | .010 | |
| Intensity-modulated RT | 26 (40) | 9 (25) | 17 (59) | ||
| Radiation dose (n = 65) | |||||
| Median (range), Gy | 30.6 (21.6-40.0) | 36 (30-40) | 30.6 (21.6-40) | ||
| >30.6 Gy | 32 (49) | 26 (72) | 6 (21) | <.001 | |
| ≤30.6 Gy | 33 (51) | 10 (28) | 23 (79) | ||
| Death | |||||
| Yes | 6 (8) | 3 (8) | 2 (7) | 1 (17) | |
| No | 65 (92) | 33 (92) | 27 (93) | 5 (83) | |
| Relapse or progression | |||||
| Yes | 15 (21) | 8 (22) | 5 (17) | 2 (33) | |
| No | 56 (79) | 28 (78) | 24 (83) | 4 (67) | |
| Local relapse | |||||
| Yes | 2 (3) | 0 | 0 | 2 (33) | |
| No | 69 (97) | 36 (100) | 29 (100) | 4 (67) | |
| Distant relapse | |||||
| Yes | 13 (18) | 8 (22) | 5 (17) | 0 | |
| No | 58 (82) | 28 (78) | 24 (83) | 6 (100) | |
| Transformation | |||||
| Yes | 2 (3) | 1 (3) | 1 (3) | .876 | 0 |
| No | 69 (97) | 35 (97) | 28 (97) | ||
| Second malignancy | |||||
| Yes | 8 (11) | 3 (8) | 5 (17) | .277 | 0 |
| No | 63 (89) | 33 (92) | 24 (83) | 6 (100) | |
| Median follow-up (95% CI), y* | 6.1 (5.0-7.2) | 6.1 (3.3-8.9) | 4.4 (0.42–8.4) | .174 | 7.5 (4.0-11.0) |
Unless otherwise noted, all data are n (%).
P value for comparison of all 3 groups is .341.
The median follow-up for all patients was 6.1 years (95% CI, 5.0-7.2), with no difference in follow-up intervals among the 3 treatment groups (P = .341; Table 3). For all patients, the 5-year rates for PFS, OS, LDFS, and DDFS were 86%, 96%, 96%, and 94%, respectively (Figure 2). There was no differences in 5-year PFS (P = .664) and OS (P = .441) among patients with stage I disease (84.3% and 95.8%, respectively) compared with stage II disease (87.3% and 96.4%, respectively). Comparing outcomes across the 3 treatment groups revealed no difference in PFS, OS, or DDFS among patients who received RT only (P = .856), systemic therapy only (P = .834), or CMT (P = .396) (Figure 3A-B,D). However, the LDFS rate was lower for patients who received systemic therapy only (5-year-LDFS rate 67%) compared with the RT-only and CMT groups (5-year LDFS rate 100% in both groups; P = .0002) (Figure 3C). Freedom from distant relapse was no different for patients treated with RT only or CMT, with 5-year DDFS rates of 93% and 95%, respectively (P = .948; Figure 3D).
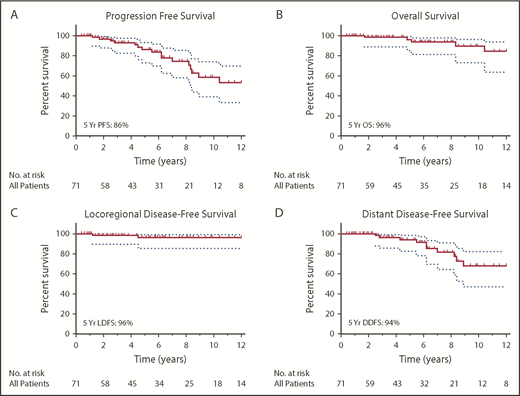
Outcomes for all patients with limited-stage NLPHL. PFS (A), OS (B), LDFS (C), and DDFS (D) among all 71 patients with stage I or stage II NLPHL treated from 1987 through 2017. Dotted lines indicate 95% CIs.
Outcomes for all patients with limited-stage NLPHL. PFS (A), OS (B), LDFS (C), and DDFS (D) among all 71 patients with stage I or stage II NLPHL treated from 1987 through 2017. Dotted lines indicate 95% CIs.
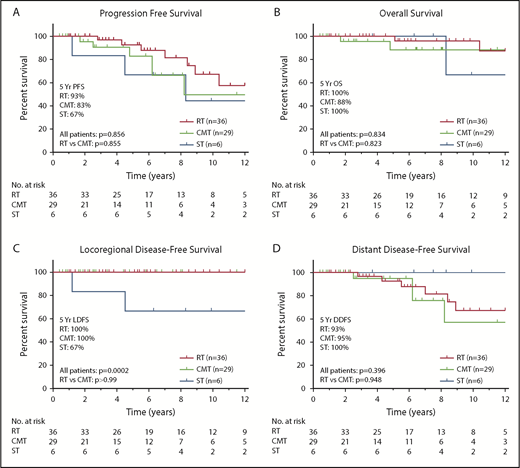
Outcomes according to treatment of patients with limited-stage NLPHL. PFS (A), OS (B), LDFS (C), and DDFS (D) for patients with stage I/II NLPHL treated with RT only (n = 36), CMT (n = 29), or systemic therapy (ST) only (n = 6).
Outcomes according to treatment of patients with limited-stage NLPHL. PFS (A), OS (B), LDFS (C), and DDFS (D) for patients with stage I/II NLPHL treated with RT only (n = 36), CMT (n = 29), or systemic therapy (ST) only (n = 6).
Fifteen patients experienced lymphoma relapse at a median of 6.2 years (range, 1.2-23.8) after initial diagnosis (Table 4); 14 of those relapses were NLPHL, and 1 had components of NLPHL and T-cell–rich DLBCL in the biopsy specimen. Regarding initial therapy among these 15 relapses, 8 were treated with RT alone, 5 were treated with CMT, and 2 were treated with systemic therapy alone. Two (13%) relapses were limited to the initial sites of nodal involvement, and both occurred in patients treated with rituximab alone (1 at 14.3 months and the other at 53.5 months). The other 13 (87%) were isolated distant relapses. No relapses involved both local and distant sites. No locoregional failures occurred among patients who received RT. The median time to local failure was 2.8 years (range, 1.2-4.5), and the median time to distant failure was 6.2 years (range, 2.5-23.8). Ten (67%) relapses occurred ≥5 years after the initial diagnosis. The relapse was located on the contralateral side of the diaphragm relative to the initial site of disease in 10 cases (67%). Two patients developed DLBCL; in both cases, the DLBCL occurred after an initial NLPHL relapse. The time from NLPHL relapse to DLBCL diagnosis was 15.2 years for 1 patient and 2.3 years for the other.
Characteristics of disease relapses according to initial therapy
| All relapses (N = 15) | RT only (n = 8) | Combined therapy (n = 5) | Systemic therapy only (n = 2) | |
|---|---|---|---|---|
| Isolated initial site | ||||
| Yes | 2 (13) | 0 | 0 | 2 (100) |
| No | 13 (87) | 8 (100) | 5 (100) | 0 |
| Isolated distant | ||||
| Yes | 13 (87) | 8 (100) | 5 (100) | 0 |
| No | 2 (13) | 0 | 2 (100) | |
| Isolated contra-diaphragmatic | ||||
| Yes | 10 (67) | 7 (88) | 3 (60) | 0 |
| No | 5 (33) | 1 (12) | 2 (40) | 2 (100) |
| Median time to relapse (range), mo | 6.2 (1.2-23.8) | 7.7 (2.8-15.7) | 6.2 (2.5-23.8) | 2.8 (1.2-4.5) |
| Relapse >5 y from diagnosis | 10 (67) | 6 (75) | 4 (80) | 0 |
| All relapses (N = 15) | RT only (n = 8) | Combined therapy (n = 5) | Systemic therapy only (n = 2) | |
|---|---|---|---|---|
| Isolated initial site | ||||
| Yes | 2 (13) | 0 | 0 | 2 (100) |
| No | 13 (87) | 8 (100) | 5 (100) | 0 |
| Isolated distant | ||||
| Yes | 13 (87) | 8 (100) | 5 (100) | 0 |
| No | 2 (13) | 0 | 2 (100) | |
| Isolated contra-diaphragmatic | ||||
| Yes | 10 (67) | 7 (88) | 3 (60) | 0 |
| No | 5 (33) | 1 (12) | 2 (40) | 2 (100) |
| Median time to relapse (range), mo | 6.2 (1.2-23.8) | 7.7 (2.8-15.7) | 6.2 (2.5-23.8) | 2.8 (1.2-4.5) |
| Relapse >5 y from diagnosis | 10 (67) | 6 (75) | 4 (80) | 0 |
Unless otherwise noted, all data are n (%).
We also examined outcomes according to radiation field size. Among the RT-only and CMT groups, PFS, LDFS, and DDFS did not differ according to RT field size (Figure 4). However, the median follow-up time was significantly shorter for patients who received ISRT in the RT-only and CMT groups. Among all 65 patients who received RT as a component of therapy, the median follow-up time was 17.9 years (95% CI, 16.7-19.0) for those who received EFRT, 8.5 years (95% CI, 6.8-10.1) for those given IFRT, and 2.6 years (95% CI, 2.0-3.2) for those treated with ISRT (P < .001).
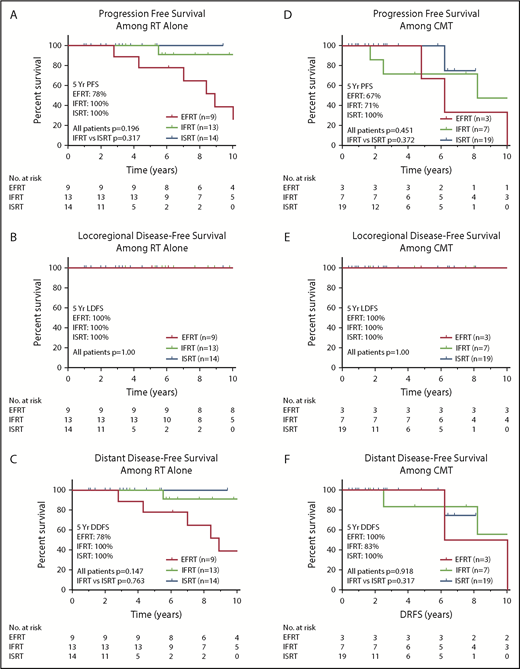
Outcomes among patients treated with RT or CMT according to radiation field size. PFS (A,D), LDFS (B,E), and DDFS (C,F) among patients treated with RT only or CMT according to field size.
Outcomes among patients treated with RT or CMT according to radiation field size. PFS (A,D), LDFS (B,E), and DDFS (C,F) among patients treated with RT only or CMT according to field size.
For the 36 patients treated with RT only, the locoregional control rate was 100%, regardless of field size (Figure 4B), and no difference was found in PFS or DDFS by field size (Figure 4A,C). PFS for the RT-only group also did not differ by radiation dose for the 10 who received ≤30.6 Gy vs the 26 who received >30.6 Gy (P = .475). PFS was also no different by RT dose among patients who received combined therapy (P = .218).
Second malignancies were diagnosed in 8 of 71 (11%) patients (2 acute myeloid leukemia [AML] and 6 solid tumors) at a median of 4.7 years from initial diagnosis (range, 1.3-13.6). Solid tumors were squamous cell carcinoma of the skin (n = 2), low-grade papillary carcinoma of the bladder (n = 1), pancreatic carcinoma (n = 1), neurogenic sarcoma (n = 1), and prostate adenocarcinoma (n = 1). No second malignancies were diagnosed in the 6 patients who received systemic therapy alone as initial therapy. Both cases of AML occurred in patients who received combined therapy (1 ABVD and 1 R-ABVD). All 6 solid tumors appeared in patients who received RT only (n = 3) or CMT (n = 3). Regarding the location of the second malignancy relative to the RT field, 1 solid second malignancy (the neurogenic sarcoma) appeared within the RT field, and the other 5 solid second malignancies were on the opposite site of the diaphragm relative to the RT field. The patient with neurogenic sarcoma developed 2 additional second malignancies during the follow-up interval: squamous cell carcinoma of the skin and melanoma. This patient had been treated with RT to 39.6 Gy with EFRT that included a mantle, para-aortic, and spleen field.
Six of 71 (8.5%) patients died a median of 6.7 years after diagnosis (range, 1.7-13.4): 1 from NLPHL transformed to DLBCL, 1 from AML, 1 from an acute cardiac arrest, and 3 from unknown causes. The 81-year-old patient who died of cardiac disease had received only IFRT to 39.6 Gy to the mediastinum and left neck 13 years earlier.
Discussion
In this single-institution series of 71 patients treated for limited-stage NLPHL over a 30-year period, outcomes were favorable across treatment approaches, with 5-year PFS and OS rates of 86% and 96%, respectively, for all patients. RT field size did not seem to affect short-term disease control, because the limited ISRT fields were equally effective as larger extended and involved fields among patients who received combined therapy or RT alone. Although it is likely that long-term tumor control is also similar, additional follow-up is required to confirm this observation. Outcomes were also equivalent with regard to disease stage (I vs II), which may reflect the merits of combined therapy. To our knowledge, this is the first analysis to evaluate treatment outcomes among patients with NLPHL treated with contemporary ISRT.
The rarity of NLPHL has precluded randomized trials of this subtype of HL; thus, data to guide treatment decisions have been derived largely from retrospective studies or larger randomized trials designed for patients with all forms of HL. The German Hodgkin Study Group (GHSG) reported outcomes for patients with stage IA NLPHL treated within prospective GHSG clinical trials at a median follow-up time of 7.6 years.13 No difference in tumor control was noted between patients treated with CMT, EFRT, or IFRT, but IFRT was associated with the smallest risk of toxicity, leading the investigators to conclude that IFRT alone should be considered the optimal treatment approach for patients with favorable stage IA disease.
In series in which limited-stage NLPHL was treated mainly with RT, having stage II disease has been reported to be associated with inferior outcomes.14,26 In a single institution series from Brigham and Women’s Hospital, 113 patients with stage I or II NLPHL received treatment between 1970 and 2005; 82% received RT alone and 12% received CMT.14 PFS estimates at 10 years were significantly inferior among patients with stage II disease (61%) compared with those with stage I NLPHL (85%; P < .006). We did not observe inferior PFS or OS among patients with stage II disease in our series, perhaps because of the increasing use of CMT for stage II NLPHL. Indeed, in our CMT subgroup, significantly greater proportions of patients had adverse features, including B symptoms and stage II NLPHL. Therefore, although we did not observe improved disease control when CMT was compared with RT only, limited conclusions can be drawn regarding the merits of CMT over RT alone, because the patients given combined therapy in this study had higher-risk disease.
Data are also limited regarding the use of systemic therapy alone for patients with early-stage NLPHL. In the GHSG series, patients with stage IA disease who received single-agent rituximab had higher relapse rates.13 Similarly, in a phase 2 trial conducted at Stanford University, 21 patients with newly diagnosed NLPHL (including 14 with stage I/II disease) were treated with single-agent rituximab.2 Although the initial overall response rate was 100%, the 5-year PFS rates were 51.9% and 41.7% for patients given or not given rituximab maintenance, respectively.2 Although only 6 patients in this study were treated with systemic therapy only, both failures in this group occurred in patients who received rituximab alone. Although the small number of patients in our study precludes drawing conclusions regarding the usefulness of traditional cytotoxic chemotherapy (R-ABVD or R-CHOP) alone for limited-stage NLPHL, it does seem that single-agent rituximab alone is insufficient. In a retrospective report of 88 patients with limited-stage NLPHL from the British Columbia Cancer Agency, 4 cycles of ABVD alone was given to 11 patients, and no relapses were observed.16 However, the investigators acknowledged the short observation time for this group and the need for additional follow-up. In the Brigham and Women’s Hospital study, of the 7 patients who received systemic therapy alone (including ABVD and older mechlorethamine-containing regimens), 4 experienced disease relapse within 2 years of initiating therapy.14 Given the limited data available at this time regarding systemic therapy alone for patients with limited-stage NLPHL, it remains unclear whether this approach will result in durable disease control.
Less aggressive treatment strategies for NLPHL are desirable, given the indolent course of the disease. The need to avoid iatrogenic complications, such as secondary neoplasia and cardiac disease, has led to increased exploration of treatment de-escalation. Historic approaches involving subtotal RT and mantle-field RT included areas of known NLPHL, as well as uninvolved nodal stations, as prophylaxis. This strategy resulted in RT exposure to the heart, lungs, and high volumes of normal tissues that led, in turn, to late mortality from cardiac disease and second malignancies.27 Although IFRT, adopted widely by many radiation oncologists in 2002, did represent a considerable reduction in field size compared with EFRT, the treated fields still covered an entire nodal region, regardless of the extent of disease involvement in that area.21 For instance, for cases in which only the mediastinum was involved, the bilateral supraclavicular fossae were treated, and the inferior border for the IFRT field was 5 cm below the carina, which would still be expected to include the proximal aspect of the coronary arteries, as well as a considerable amount of cardiac tissue. Indeed, for patients with disease in a limited aspect of the neck, IFRT fields would extend from the base of the skull to 2 cm below the clavicle. In contrast, contemporary ISRT treatment approaches, as established by the International Lymphoma Radiation Oncology Group, are designed to target initially involved lymph nodes with a margin for differences in set-up between the initial diagnostic CT images and the RT treatment position.22 For practitioners who have the ability to do pretherapy PET-CT imaging in the RT treatment position, involved nodal radiation therapy would permit even smaller RT fields as a result of the reduced set-up margins.28,29 ISRT fields would be expected to result in a substantial reduction in treatment toxicity for patients with NLPHL in particular, because the mediastinum is infrequently involved, and ISRT fields would rarely involve irradiation of the heart and lungs. Further, given the male predominance of NLPHL, secondary breast cancer would be less of a concern, even when the axilla is targeted.
Several studies have evaluated the efficacy of EFRT vs IFRT alone for patients with limited-stage NLPHL. In a series by Wirth et al from Australia, in which 146 patients with nonmediastinal disease above the diaphragm were treated with RT alone, more limited IFRT fields did not adversely affect disease control.26 In the study reported from the Brigham and Women's Hospital, of 106 patients who received RT for early-stage NLPHL, PFS and OS did not differ based on treatment with limited-field, regional-field, or extended-field RT.14 The investigators defined “limited field” as IFRT, “regional field” as mantle or para-aortic RT, and “extended field” as total nodal or subtotal nodal RT. In the current study, we did not observe an increase in disease relapse with ISRT. We acknowledge that treating NLPHL with RT alone may lead to some trepidation when RT field sizes are limited to areas of radiographic gross disease with limited margins, out of concern for inadvertent omission of regional microscopic disease. This concern probably influenced treatment decisions for patients in our study, because a smaller proportion of patients treated with RT alone had stage II disease compared with those treated with combined therapy. In addition, to our knowledge, few studies reporting on outcomes in early-stage NLPHL patients have included diagnostic PET-CT imaging.14,15,26 In previous studies of patients treated primarily with RT alone, the extent of disease at diagnosis could have been underestimated owing to the lack of PET-CT imaging, which could account for inferior outcomes among patients with stage II disease. Indeed, in this study, 85% of patients had PET-CT imaging at diagnosis, and a lack of PET-CT imaging at diagnosis was associated with inferior PFS.
Currently acceptable RT doses for NLPHL therapy range from 30 to 40 Gy. In the current study, roughly half of the patients who received RT received doses ≤30.6 Gy. In the RT-only subgroup, 28% of patients received a dose of 30 to 30.6 Gy, but no patient received a dose <30 Gy. Nevertheless, the locoregional control rate was 100% among all patients treated with RT, regardless of the RT dose given, suggesting that even doses <30 Gy may be effective, as is the case for certain subtypes of indolent B-cell lymphoma (eg, follicular lymphoma and marginal zone lymphoma), for which 24 Gy is adequate to treat gross disease.30 In GHSG trial HD10, in which 2 cycles of ABVD and 20 Gy of IFRT were found to be as effective, but less toxic, than 4 cycles of ABVD and 30 Gy, 7.5% of patients (n = 81) had NLPHL.31 These data suggest that 20 Gy is adequate for early-stage favorable NLPHL patients who receive systemic therapy before consolidative RT. Furthermore, in a study examining the efficacy of ultralow-dose RT with a dose of 4 Gy among 9 patients with NLPHL, the overall response rate was 89% after a median follow-up of 37 months.32 Six patients achieved a complete remission; however, local relapse was not uncommon, occurring in 5 of 8 evaluable patients. Additional studies may shed light on the lowest oncologically effective dose of RT.
Second neoplasia and cardiac toxicity are important concerns for patients receiving RT, especially those treated with older RT techniques and extended fields. In a series of patients treated for NLPHL from 1970 to 1993, of whom 61 of 71 received RT alone with extended fields, including mantle-field RT, subtotal nodal irradiation, or total nodal irradiation, 9 of 71 patients died with a median follow-up time of 10.8 years; only 1 of these patients died from NLPHL.27 Five patients died from second cancers, and 2 patients died from cardiac disease. The authors concluded that less aggressive therapy may lower the risk of long-term complications. In the current study, 2 patients died from causes related to second cancers, and 1 died from cardiac disease. One of the second-cancer deaths occurred in a patient treated with EFRT, and the cardiac death occurred in 1 of the few patients who received RT to the mediastinum who was treated with IFRT. Limiting normal tissue exposure via RT field reduction has been shown to reduce second-cancer risk; therefore, reducing the RT field size has important implications for limiting iatrogenic complications among patients with early-stage NLPHL.33
This study had limitations beyond its retrospective nature. Follow-up for patients treated with ISRT was significantly shorter than that for patients treated with EFRT or IFRT. Additional follow-up is required to confirm continued locoregional disease control with the additional field size reduction from IFRT to ISRT, especially for patients who received ISRT as the sole therapy. Furthermore, treatment approaches were not assigned, introducing the potential for confounding bias. As a result, more stage II patients were treated with combined therapy; thus, our ability to conclude that stage II NLPHL may be adequately treated with RT alone is limited in the absence of additional data. Finally, relatively few patients were treated with immunochemotherapy alone; therefore, the potential merits of this treatment approach could not be adequately assessed.
Despite its shortcomings, this study adds to the existing literature indicating favorable outcomes for patients with limited-stage NLPHL, for whom death from NLPHL or transformed disease is rare. The strengths of our study include the detailed follow-up over 3 decades, the central pathology review, and the use of modern PET-CT for staging in most cases. In this initial report on the use of contemporary ISRT treatment fields, disease control was not affected by RT field size, with 100% locoregional control achieved among all patients who received RT alone or combined RT and systemic therapy. This study contributes to the growing body of literature suggesting that the pursuit of less aggressive treatment strategies is warranted for patients who are vulnerable to late treatment–related toxicity.
Acknowledgment
This work was supported in part by Cancer Center Support (Core) Grant CA016672 from the National Cancer Institute, National Institutes of Health to The University of Texas MD Anderson Cancer Center.
Authorship
Contribution: C.C.P., S.A.M., C.Y.C., J.R.G., and B.S.D. designed the research, collected the data, analyzed the data, and wrote the manuscript; E.B.L. analyzed the data and wrote the manuscript; L.J.M. and A.E.R. collected the data and wrote the manuscript; L.J.N., S.S.N., J.W., H.J.L., S.P.I., R.E.S., L.E.F., N.H.F., M.L.W., F.S., and M.A.R. designed the research and wrote the manuscript; and C.F.W. wrote the manuscript.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Chelsea C. Pinnix, Department of Radiation Oncology, Unit 97, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX 77030; e-mail: ccpinnix@mdanderson.org.

