

Key Points
Patients with t-MDS are underrepresented in clinical trials when taking into account the prevalence of such patients.
Eligibility criteria and sponsorship type may contribute to t-MDS patient exclusion.

Abstract
Therapy-related myelodysplastic syndrome (t-MDS), defined as MDS occurring after previous exposure to chemotherapy or radiotherapy, constitutes 10% to 20% of all MDS diagnoses. t-MDS patients tend to have higher-risk disease and worse outcomes than de novo MDS patients and are often excluded from therapeutic clinical trials. To explore this further, we extracted clinical trials across all status types registered on ClinicalTrials.gov from 1999 to 2018 studying untreated MDS patients. Using these specific search criteria, we analyzed 317 therapeutic MDS trials based on study status, therapeutic indication, eligibility criteria, and sponsor type to examine if these factors influenced t-MDS patient inclusion. Only 18 studies (5.7%) accrued 231 t-MDS patients in total, representing 3.2% of the total accrued MDS trial patient population. Fewer t-MDS patients were accrued in therapeutic trials sponsored by pharmaceutical sponsors vs nonpharmaceutical sponsors (2.8% vs 4.0%; P = .0073). This pattern of exclusion continues in actively enrolling trials; only 5 (10%) of 49 studies specifically mention the inclusion of t-MDS patients in their eligibility criteria. Our results indicate that therapeutic MDS trials seem to exclude t-MDS patients, rendering study results less applicable to this subset of MDS patients, who often have poor outcomes. Our study emphasizes the importance of the recent focus by National Cancer Institute cooperative groups and societies to broaden eligibility criteria for all patients.
Introduction
Myelodysplastic syndromes (MDSs) are hematologic disorders characterized by morphologic dysplasia and ineffective hematopoiesis and became reportable as malignancies in the Surveillance, Epidemiology, and End-Results program in 2001.1 These neoplasms are reported as either de novo, secondary, or familial.2 Patients with a history of cancer treatment, environmental exposure, inherited genetic abnormalities such as Fanconi anemia, or hematologic disorders such as paroxysmal nocturnal hemoglobinuria are placed in the secondary MDS category.3
Therapy-related MDS (t-MDS), a subtype of secondary MDS and therapy-related neoplasms per the 2016 World Health Organization (WHO) classification, is defined as MDS occurring after previous exposure to chemotherapy or radiotherapy administered for other disease indications. It constitutes ∼10% to 20% of all MDS cases.1,4,,,-8 The incidence rate of t-MDS is estimated to increase by 2% annually as a result of increased use of chemotherapy and radiotherapy and extended survival of patients with prior malignancies treated with these modalities.9
Exposure to any cytotoxic or radiation anticancer therapy leads to a 0.24% to 5.4% lifetime risk of developing t-MDS.4,9,10 Other factors, including preexisting somatic or germ line mutations, age at diagnosis, and smoking history, further increase this risk.4 Compared with de novo MDS patients, those with t-MDS present with a higher frequency of high-risk genetic abnormalities or bone marrow blasts,4,10 leading to worse overall survival (19 months) than that of de novo MDS patients (46 months).11
Recognizing, reporting, and properly categorizing t-MDS vs secondary MDS can be challenging. Patients with a history of chemotherapy or radiotherapy for another cancer may present with MDS that is coincidentally de novo (eg, del20q and DNMT3A mutation as the only clonal drivers), whereas others without such a therapy history are likely to have exposure-related MDS based upon their presentation with a complex karyotype, TP53 mutations, and other characteristics more frequently seen in patients with therapy-related disease.4,12 Secondly, the latency period between exposure and development of t-MDS is variable, ranging from <2 years to a decade or more.4,12
Ideally, a clinical trial should generate evidence supporting the use of novel therapies applicable across broad patient populations. Clinical trials, particularly those sponsored by pharmaceutical companies, tend to design eligibility criteria that result in recruitment of homogenous, lower-risk, healthier patient populations.8,13,,,-17 This may lead to approval of drugs unable to produce equitable benefits across diverse patient populations, particularly those who are older or have organ dysfunction or comorbidities. t-MDS patients have also been underrepresented in the development of widely used prognostic scoring systems to risk stratify MDS patients, which are used for trial eligibility.4,11
Although the underrepresentation of t-MDS patients accrued to therapeutic MDS clinical trials has been acknowledged, the degree to which t-MDS patients are excluded from trials and relationship between clinical trial eligibility criteria and t-MDS accrual have not been previously explored. We categorized the t-MDS eligibility criteria for therapeutic MDS clinical trials, evaluated the association between these criteria and t-MDS accrual over a 20-year period, and identified whether trial characteristics, such as sponsor type, were associated with disproportionate exclusion of t-MDS patients.
Methods
Data sources and searches
We performed a search to identify all therapeutic MDS clinical trials for adults (age >18 years) registered on ClinicalTrials.gov between 1 November 1999 and 10 August 2018 using the following search terms: myelodysplastic syndromes, phase 2, phase 3, adult, and MDS. This included all completed, actively recruiting, ongoing but not recruiting, terminated, and suspended trials. Study title, phase, study type, treatment regimen, inclusion criteria, exclusion criteria, and primary/secondary objectives were reviewed for all clinical trials.
Clinical trials were included if they enrolled at least 1 cohort of adult (>18 years of age) newly diagnosed, untreated MDS patients; used the WHO or French-American-British system to classify the MDS diagnosis (defined as refractory anemia [RA], refractory cytopenia with multilineage dysplasia, RA with ring sideroblasts, or RA with excess blasts [RAEB-1 or RAEB-2] per WHO or RA, RA with ring sideroblasts, or RAEB per French-American-British); studied MDS patients in any risk category as determined by the International Prognostic Scoring System (low, intermediate-1/2, or high-risk) or revised International Prognostic Scoring System (very low, low, intermediate, high, or very high); confirmed diagnoses via cytogenic testing, bone marrow examination, and/or routine laboratory testing; and studied MDS patient outcomes in response to chemotherapy or growth factors such as erythropoietin stimulating agents or thrombopoietin.
Clinical trials were excluded if they examined pediatric patients (<18 years of age), conditioning regimens or post–allogeneic stem cell transplantation therapy, expanded access programs, acute myeloid leukemia (AML) or AML transformation to MDS, chronic myelomonocytic leukemia (CMML), hypoplastic MDS, prophylaxis, iron chelation therapy, dietary supplementation, vaccination, emesis reduction, graft-versus-host disease, quality-of-life measurement, QTc prolongation, molecular research, maintenance therapy, or salvage therapy or if trial status was no longer available.
Data extraction
We extracted the following variables from the included trials: ClinicalTrials.gov identifier, study title, study drug, phase, inclusion /exclusion criteria, when the study was first received and last updated, MDS subtype and classification, sponsor, collaborators, target enrollment, actual enrollment, start date and completion date, status of the study (ie, completed, not yet recruiting, ongoing but not recruiting, recruiting, terminated, suspended recruitment, withdrawn before enrollment, or unknown), study type, and name/contact information of primary investigator if available. A clinical trial was categorized as unknown if the status or results had not been updated for >2 years after the estimated completion date.
Clinical trials that matched inclusion criteria were classified into 3 groups based on eligibility criteria: group A, trials that excluded patients with secondary or t-MDS specifically by mentioning “exclusion of patients with t-MDS or secondary MDS” in the exclusion criteria; group B, trials that did not indicate exclusion or inclusion of secondary or t-MDS patients, did not contain any language in the exclusion or inclusion criteria found in group A or C, and contained language similar or identical to “a history of previous malignancy unless patient has been disease free” for >1 to 5 years; and group C, trials that specifically included secondary or t-MDS patients in the eligibility criteria by mentioning “inclusion of patients with t-MDS or secondary MDS” in the inclusion criteria.
It is important to note that the clinical trial eligibility criteria used the terms secondary MDS or t-MDS. As mentioned in the Introduction, there are multiple subtypes of secondary disease, such as exposure-related or familial MDS. Because these subtypes are rare and/or were not mentioned in all of the eligibility criteria per ClinicalTrials.gov, secondary MDS and t-MDS will be used interchangeably throughout the rest of this work.
For all clinical trials categorized into group B, ClinicalTrials.gov was used to identify eligibility criteria. If available, the maximum age of inclusion, performance status, and organ function levels (eg, serum creatinine, aminotransferase, or bilirubin) were collected. Furthermore, the number of trials that excluded patients with a history of hepatitis, HIV, uncontrolled hypertension, autoimmune diseases, pneumonitis, and chronic kidney disease were quantified and compared across status type.
Each clinical trial belonging to group A, B, or C was further categorized based on phase (1/2, 2/3, 2, or 3), study drug, status of the trial, and sponsor. Study drug categories included hypomethylating agents, novel agents, growth factors, and US Food and Drug Administration–approved oral chemotherapeutic agents; a study drug was classified as other if it did not fall into 1 of the 4 categories.
Using Google Scholar, PubMed, or Google, full manuscripts or abstracts were searched for clinical trials across all groups that met inclusion criteria and were marked as completed, ongoing, unknown, or terminated. Trials with these statuses were more likely to have been published or be in the process of publishing study results. Both full manuscripts and abstracts were included in an effort to capture both positive and negative studies. Key words from the clinical trial title, ClinicalTrials.gov identification number, year of termination, author, and accrual were used to match the clinical trial with its publication. Abstracts from conferences were obtained from the Web site archives of the American Society of Hematology, American Society of Clinical Oncology (ASCO), and European Hematology Association. Manuscripts were obtained from journals when trial results were reported in their entirety.
Each publication (manuscript or abstract) was reviewed to validate the information in ClinicalTrials.gov and allow for the abstraction of enrollment and accrual details if not updated or reported on ClinicalTrials.gov. In particular, the patient eligibility portion of the methods section was reviewed to assess whether the inclusion/exclusion criteria in the publication were similar to the language of the trial found on ClinicalTrials.gov.
Secondly, the results section, specifically the patient characteristic section, was reviewed to identify whether patients with secondary MDS were accrued or not and if the authors mentioned what type of secondary MDS. It was noted whether the authors mentioned the type of therapy the patients with t-MDS had received, such as chemotherapy and/or radiotherapy, transplantation, or surgery. The conclusion section was assessed for discussion on outcomes regarding t-MDS or de novo or secondary MDS. Searches were performed of each abstract or manuscript for key terms such as t-MDS, secondary, therapy, or therapy related to ensure important information regarding t-MDS patients was captured.
Finally, published clinical trials were sorted by sponsor type. A trial sponsored by a pharmaceutical company was defined as any trial sponsored by a pharmaceutical company individually or by a cooperative group in collaboration with a pharmaceutical company. A clinical trial sponsored by a comprehensive cancer center and funded by the National Cancer Institute (NCI) or any of the cooperative groups was categorized as having a nonpharmaceutical sponsor.
Statistical analysis
Trial characteristics were summarized using descriptive statistics and by t-MDS patient eligibility group. To evaluate whether t-MDS patients were underrepresented in a clinical trials, 1-sample proportion test was used to compare the proportion of t-MDS patients in the trials with the prevalence of t-MDS patients among the general population of MDS patients. Prevalence was conservatively assumed to be 10%, given the literature reported 10% to 20%.1,4,,,-8 The association between trial phase type, therapeutic investigation, disease focus, eligibility group status, trial sponsorship, and accrual of t-MDS patients in therapeutic clinical trials was evaluated using the χ2 test or Fisher’s exact test as appropriate. Two-sided P < .05 denoted significance.
Results
Characteristics of clinical trials
Our initial search yielded 1148 trials; 831 trials were excluded from additional analyses because they did not match the inclusion criteria outlined in “Methods.” Of the remaining 317 included trials, 15% (n = 46) were classified as group A (trials excluding patients with t-MDS), 77% (n = 244) as group B (trials not indicating exclusion or inclusion of t-MDS patients), and 9% (n = 27) as group C (trials specifically including t-MDS patients). Groups A and B had clinical trials across all status types, whereas group C did not have any trials with status marked as withdrawn before enrollment or not yet recruiting (Table 1). Phase 1/2 clinical trials were statistically more common than 2/3 (P < .0001) across all 3 groups as well as trials studying solely MDS as compared with trials studying MDS, AML, and CML (P < .001; Table 2). Oral chemotherapy and hypomethylating agents were most commonly investigated across all 3 groups (P = .004). All 3 groups had similar proportions of completed, ongoing and recruiting, terminated, withdrawn, unknown, and currently recruiting studies (P = .971; Table 2).
Clinical trial characteristics sorted by groups A, B, and C
| Group A (n = 46), n (%) | Group B (n = 244), n (%) | Group C (n = 27), n (%) | Total (N = 317), n (%) | |
|---|---|---|---|---|
| Phase | ||||
| 1/2 | 7 (15.3) | 50 (20.0) | 2 (7.4) | 59 (19.0) |
| 2 | 25 (54.3) | 173 (71.0) | 22 (81.5) | 220 (69.0) |
| 2/3 | 2 (4.3) | 4 (2.0) | 1 (3.7) | 7 (2.0) |
| 3 | 12 (26.1) | 17 (7.0) | 2 (7.4) | 31 (10.0) |
| Status | ||||
| Completed | 20 (43.5) | 116 (47.0) | 12 (44.5) | 148 (47.0) |
| Terminated | 5 (10.9) | 36 (15.0) | 5 (18.5) | 46 (15.0) |
| Ongoing | 6 (13.0) | 21 (9.0) | 2 (7.4) | 29 (9.0) |
| Unknown | 6 (13.0) | 22 (9.0) | 3 (11.1) | 31(10.0) |
| Recruiting | 5 (10.9) | 39 (16.0) | 5 (18.5) | 49 (15.0) |
| Withdrawn before enrollment | 3 (6.5) | 7 (3.0) | 0 (0.0) | 10 (3.0) |
| Not yet recruiting | 1 (2.2) | 3 (1) | 0 (0.0) | 4 (1.0) |
| Disease focus | ||||
| MDS only | 44 (95.7) | 148 (61.0) | 19 (70.3) | 211 (67.0) |
| AML, CMML, or other hematologic malignancies | 2 (4.3) | 96 (39.0) | 8 (29.7) | 106 (33.0) |
| Therapy used | ||||
| HMAs | 7 (15.2) | 67 (27.0) | 12 (44.4) | 86 (27.0) |
| Novel agents | 5 (10.9) | 30 (13.0) | 2 (7.4) | 37 (12.0) |
| Growth factors | 17 (37.0) | 29 (12.0) | 2 (7.4) | 48 (15.0) |
| Oral Chemotherapy | 13 (28.3) | 76 (31.0) | 9 (33.3) | 98 (31.0) |
| Others | 4 (8.7) | 42 (17.0) | 2 (7.4) | 48 (15.0) |
| Group A (n = 46), n (%) | Group B (n = 244), n (%) | Group C (n = 27), n (%) | Total (N = 317), n (%) | |
|---|---|---|---|---|
| Phase | ||||
| 1/2 | 7 (15.3) | 50 (20.0) | 2 (7.4) | 59 (19.0) |
| 2 | 25 (54.3) | 173 (71.0) | 22 (81.5) | 220 (69.0) |
| 2/3 | 2 (4.3) | 4 (2.0) | 1 (3.7) | 7 (2.0) |
| 3 | 12 (26.1) | 17 (7.0) | 2 (7.4) | 31 (10.0) |
| Status | ||||
| Completed | 20 (43.5) | 116 (47.0) | 12 (44.5) | 148 (47.0) |
| Terminated | 5 (10.9) | 36 (15.0) | 5 (18.5) | 46 (15.0) |
| Ongoing | 6 (13.0) | 21 (9.0) | 2 (7.4) | 29 (9.0) |
| Unknown | 6 (13.0) | 22 (9.0) | 3 (11.1) | 31(10.0) |
| Recruiting | 5 (10.9) | 39 (16.0) | 5 (18.5) | 49 (15.0) |
| Withdrawn before enrollment | 3 (6.5) | 7 (3.0) | 0 (0.0) | 10 (3.0) |
| Not yet recruiting | 1 (2.2) | 3 (1) | 0 (0.0) | 4 (1.0) |
| Disease focus | ||||
| MDS only | 44 (95.7) | 148 (61.0) | 19 (70.3) | 211 (67.0) |
| AML, CMML, or other hematologic malignancies | 2 (4.3) | 96 (39.0) | 8 (29.7) | 106 (33.0) |
| Therapy used | ||||
| HMAs | 7 (15.2) | 67 (27.0) | 12 (44.4) | 86 (27.0) |
| Novel agents | 5 (10.9) | 30 (13.0) | 2 (7.4) | 37 (12.0) |
| Growth factors | 17 (37.0) | 29 (12.0) | 2 (7.4) | 48 (15.0) |
| Oral Chemotherapy | 13 (28.3) | 76 (31.0) | 9 (33.3) | 98 (31.0) |
| Others | 4 (8.7) | 42 (17.0) | 2 (7.4) | 48 (15.0) |
HMA, hypomethylating agent.
Analytical comparison of clinical trial characteristics across groups A, B, and C
| Group A, n | Group B, n | Group C, n | Total, N | P* | |
|---|---|---|---|---|---|
| Phase | <.001† | ||||
| 1/2 or 2 | 32 | 223 | 24 | 279 | |
| 2/3 or 3 | 14 | 21 | 3 | 38 | |
| Status | .971 | ||||
| Completed | 20 | 116 | 12 | 148 | |
| Ongoing or recruiting | 11 | 60 | 7 | 78 | |
| Terminated, withdrawn, unknown, or not yet recruiting | 15 | 68 | 8 | 91 | |
| Disease focus | <.001† | ||||
| MDS only | 44 | 148 | 19 | 211 | |
| AML, CMML, or other hematologic malignancies | 2 | 96 | 8 | 106 | |
| Therapy used | .004† | ||||
| HMAs | 7 | 67 | 12 | 86 | |
| Novel agents | 5 | 30 | 2 | 37 | |
| Growth factors | 17 | 29 | 2 | 48 | |
| Oral chemotherapy | 13 | 76 | 9 | 98 | |
| Others | 4 | 42 | 2 | 48 |
| Group A, n | Group B, n | Group C, n | Total, N | P* | |
|---|---|---|---|---|---|
| Phase | <.001† | ||||
| 1/2 or 2 | 32 | 223 | 24 | 279 | |
| 2/3 or 3 | 14 | 21 | 3 | 38 | |
| Status | .971 | ||||
| Completed | 20 | 116 | 12 | 148 | |
| Ongoing or recruiting | 11 | 60 | 7 | 78 | |
| Terminated, withdrawn, unknown, or not yet recruiting | 15 | 68 | 8 | 91 | |
| Disease focus | <.001† | ||||
| MDS only | 44 | 148 | 19 | 211 | |
| AML, CMML, or other hematologic malignancies | 2 | 96 | 8 | 106 | |
| Therapy used | .004† | ||||
| HMAs | 7 | 67 | 12 | 86 | |
| Novel agents | 5 | 30 | 2 | 37 | |
| Growth factors | 17 | 29 | 2 | 48 | |
| Oral chemotherapy | 13 | 76 | 9 | 98 | |
| Others | 4 | 42 | 2 | 48 |
Fisher’s exact test.
Denotes significance at P < .05.
After analysis of completed, terminated, unknown, and ongoing trials, 129 trials were found to have publications; 14.8% (n = 19) were classified as group A, 73.4% (n = 95) were classified as group B, and 11.7% (n = 15) were classified as group C (Figure 1). These proportions were similar to those for all included trials, regardless of publication availability.
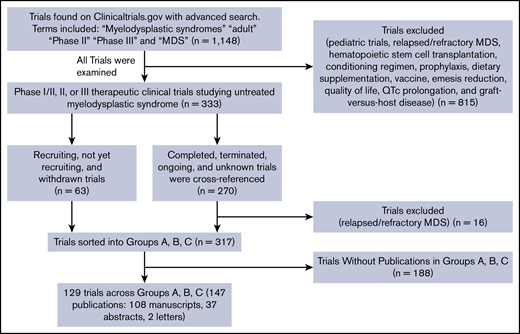
Flow diagram outlining the selection process of MDS trials. Group A trials excluded t-MDS patients, group B mentioned neither the exclusion nor inclusion of t-MDS patients, and group C trials included t-MDS patients.
Flow diagram outlining the selection process of MDS trials. Group A trials excluded t-MDS patients, group B mentioned neither the exclusion nor inclusion of t-MDS patients, and group C trials included t-MDS patients.
The eligibility criteria on ClinicalTrials.gov were examined in the group B trials with publications (n = 95) as well as status marked as recruiting (n = 39; Table 3). Eighty-five (63%) mentioned the exclusion of patients with an Eastern Cooperative Oncology Group performance score >2. Eighty-nine trials (66%) excluded patients based on renal function status, 88 trials (65%) excluded based on transaminase levels, and 47 trials (35%) excluded patients with heart failure. Notably, 41 trials (30%) excluded patients with a history of or active hepatitis infection, whereas 56 (42%) excluded patients with HIV infection.
Eligibility criteria characteristics for published and recruiting trials belonging to trials in group B
| Exclusion criteria | With publication (n = 95), n* | Recruiting (n = 39), n | Total (N = 134), N |
|---|---|---|---|
| Maximum age, y | |||
| 59-69 | 3 | 3 | 6 |
| 70-89 | 5 | 0 | 5 |
| 90-100 | 1 | 0 | 1 |
| ECOG PS | |||
| 1 | 3 | 2 | 5 |
| 2 | 60 | 25 | 85 |
| 3 | 5 | 3 | 8 |
| Creatinine (<ULN), mg/dL | |||
| 1.0-1.5 | 16 | 13 | 29 |
| 2.0-2.5 | 41 | 17 | 58 |
| >3 | 2 | 0 | 2 |
| ALT or AST (×ULN), U/L | |||
| 1.0-1.5 | 1 | 0 | 1 |
| 2.0-2.5 | 29 | 19 | 48 |
| >3.0 | 25 | 14 | 39 |
| Total bilirubin (×ULN), mg/dL | |||
| 1.0-1.5 | 26 | 16 | 42 |
| 2.0-2.5 | 27 | 15 | 42 |
| >3.0 | 4 | 1 | 5 |
| Heart failure (any grade) | 29 | 18 | 47 |
| History of or active hepatitis | 20 | 21 | 41 |
| Diagnosis of HIV | 30 | 26 | 56 |
| Uncontrolled HTN | 14 | 3 | 17 |
| Autoimmune disease | 4 | 1 | 5 |
| Diabetes mellitus | 1 | 1 | 2 |
| Chronic kidney disease | 1 | 1 | 2 |
| History of pneumonitis | 0 | 3 | 3 |
| Exclusion criteria | With publication (n = 95), n* | Recruiting (n = 39), n | Total (N = 134), N |
|---|---|---|---|
| Maximum age, y | |||
| 59-69 | 3 | 3 | 6 |
| 70-89 | 5 | 0 | 5 |
| 90-100 | 1 | 0 | 1 |
| ECOG PS | |||
| 1 | 3 | 2 | 5 |
| 2 | 60 | 25 | 85 |
| 3 | 5 | 3 | 8 |
| Creatinine (<ULN), mg/dL | |||
| 1.0-1.5 | 16 | 13 | 29 |
| 2.0-2.5 | 41 | 17 | 58 |
| >3 | 2 | 0 | 2 |
| ALT or AST (×ULN), U/L | |||
| 1.0-1.5 | 1 | 0 | 1 |
| 2.0-2.5 | 29 | 19 | 48 |
| >3.0 | 25 | 14 | 39 |
| Total bilirubin (×ULN), mg/dL | |||
| 1.0-1.5 | 26 | 16 | 42 |
| 2.0-2.5 | 27 | 15 | 42 |
| >3.0 | 4 | 1 | 5 |
| Heart failure (any grade) | 29 | 18 | 47 |
| History of or active hepatitis | 20 | 21 | 41 |
| Diagnosis of HIV | 30 | 26 | 56 |
| Uncontrolled HTN | 14 | 3 | 17 |
| Autoimmune disease | 4 | 1 | 5 |
| Diabetes mellitus | 1 | 1 | 2 |
| Chronic kidney disease | 1 | 1 | 2 |
| History of pneumonitis | 0 | 3 | 3 |
Group B comprises trials that neither included nor excluded t-MDS patients.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; ECOG PS, Eastern Cooperative Oncology Group performance score; HTN, hypertension; ULN, upper limit of normal.
Data are specific to published works with a status marked as completed, terminated, ongoing, or unknown as well as recruiting trials.
When examining all trials without clear t-MDS inclusion/exclusion criteria (group B), 76 trials (31%) excluded patients with a history of prior malignancy; of these, 1 (1%) excluded patients with a prior malignancy within <1 year, 19 (25%) within the past 1 year, 12 (16%) within the past 2 years (16%), 30 (40%) within the past 3 years, and 14 (18%) within the past 5 years.
t-MDS patient accrual
The 129 published trials accrued 7178 MDS patients; a majority of trials (n = 89) were categorized as completed and accrued 4939 participants (Table 4). Of the 129 trials, 128 (comprising 7172 MDS patients) reported whether or not t-MDS patients were included in the study. One publication was excluded because the results section did not specify the origin of secondary disease (MDS or AML).18
t-MDS and MDS patient accrual in published clinical trials
| Patient accrual | Group A, n | Group B, n | Group C, n | Total, N |
|---|---|---|---|---|
| Completed trials (n = 4939) | ||||
| t-MDS | 0 | 143 | 35 | 178 |
| MDS | 1138 | 3299 | 502 | 4939 |
| Ongoing trials (n = 1183) | ||||
| t-MDS | 0 | 18 | 0 | 18 |
| MDS | 182 | 1001 | 0 | 1183 |
| Terminated trials (n = 313) | ||||
| t-MDS | 0 | 2 | 3 | 5 |
| MDS | 47 | 212 | 54 | 313 |
| Unknown trials (n = 737) | ||||
| t-MDS | 0 | 1 | 29 | 30 |
| MDS | 194 | 312 | 231 | 737 |
| Patient accrual | Group A, n | Group B, n | Group C, n | Total, N |
|---|---|---|---|---|
| Completed trials (n = 4939) | ||||
| t-MDS | 0 | 143 | 35 | 178 |
| MDS | 1138 | 3299 | 502 | 4939 |
| Ongoing trials (n = 1183) | ||||
| t-MDS | 0 | 18 | 0 | 18 |
| MDS | 182 | 1001 | 0 | 1183 |
| Terminated trials (n = 313) | ||||
| t-MDS | 0 | 2 | 3 | 5 |
| MDS | 47 | 212 | 54 | 313 |
| Unknown trials (n = 737) | ||||
| t-MDS | 0 | 1 | 29 | 30 |
| MDS | 194 | 312 | 231 | 737 |
Of 7172 MDS patients enrolled in 128 published trials, 231 (3.2%) of enrolled MDS patients had t-MDS. This was significantly lower than the reported prevalence of t-MDS patients in the general MDS patient population (P < .0001).
When sorted by group assignment, group A trials recruited no t-MDS patients by definition. A small percentage of trials recruited t-MDS patients in groups B and C; 164 t-MDS patients were accrued in group B, and 67 t-MDS patients were accrued in group C, as shown in Table 3, with t-MDS accrual per group ranging from 3% to 7% (Figure 2).
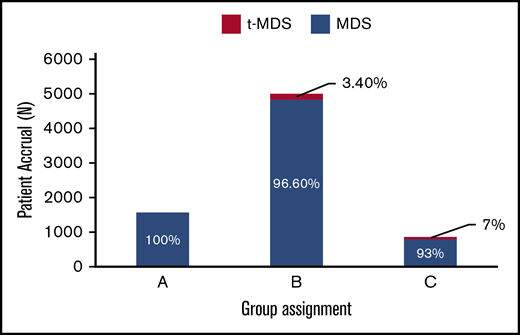
Comparison of MDS and t-MDS patient accrual across groups A, B, and C. The patient accrual on the y-axis represents the MDS and t-MDS patients who were accrued in trials that also had affiliated published works (either abstract or manuscript) within the past 20 years. Group A trials excluded t-MDS patients, group B mentioned neither the exclusion nor inclusion of t-MDS patients, and group C trials included t-MDS patients.
Comparison of MDS and t-MDS patient accrual across groups A, B, and C. The patient accrual on the y-axis represents the MDS and t-MDS patients who were accrued in trials that also had affiliated published works (either abstract or manuscript) within the past 20 years. Group A trials excluded t-MDS patients, group B mentioned neither the exclusion nor inclusion of t-MDS patients, and group C trials included t-MDS patients.
t-MDS accrual specific to groups B and C
When examining the published manuscripts or abstracts of the 95 group B published trials, 94 of the publications indicated whether or not t-MDS patients were accrued. Although the eligibility criteria of group B addressed neither the inclusion nor exclusion of t-MDS patients in the study, further examination of group B publications revealed that t-MDS patients were accrued in 14.8% of 94 published trials (n = 14; 11 completed, 1 ongoing, 1 terminated, and 1 unknown). Of 14 publications, 3 specified the inclusion of t-MDS patients and what type of previous treatment they had received. The remaining 11 trials included t-MDS patients but did not specify what type of therapy the patients had received.
Two of the 14 trials had conclusions referencing t-MDS outcomes compared with those of de novo MDS patients; both were completed phase 2 trials with published manuscripts.19,20 The first, which studied alisertib (MLN8237), accrued 1 t-MDS patient who showed no response to therapy.20 The second trial, which studied low-dose decitabine with or without valproic acid, accrued 34 patients with t-MDS and concluded that patients with t-MDS did not have improved outcomes compared with de novo patients.19
Of the remaining 12 trials accruing t-MDS patients in group B (9 completed, 1 terminated, 1 ongoing, and 1 unknown), 6 mentioned secondary MDS in the patient characteristics section of a published manuscript or abstract but did not mention t-MDS patient outcomes in results or conclusion sections.21,,,,,,,-29 Three mentioned the therapy history of the t-MDS patients in patient characteristics sections but did not mention t-MDS outcomes in results or conclusion sections.22,25,26
The ongoing trial recruiting t-MDS patients has accrued 18 patients,30 whereas the terminated trial recruited 2 t-MDS patients,31 and the unknown trial recruited 1 t-MDS patient.32
Of the 15 published group C trials (3 abstracts, 12 manuscripts), only 26.6% (n = 4; 1 terminated, 2 completed, and 1 unknown) actually accrued t-MDS patients.33,-35 One completed study recruited 6 t-MDS patients, studied azacitidine, and mentioned the patients’ prior therapeutic history (2 patients received prior chemotherapy, 3 received prior radiotherapy, and 1 received both).33 The 1 terminated trial recruited 3 secondary MDS patients and studied sorafenib.34 Neither made conclusions regarding outcomes of these patients.30,31
The other completed study examined the use of azacitidine with or without entinostat in 29 t-MDS patients and described the patient exposure history of all patients with therapy-related neoplasms included in the study but did not specify exposure for t-MDS patients specifically. No significant differences were seen in overall response rates or outcomes for t-MDS vs de novo MDS patients.35 Lastly, a study with clinical trial status marked as unknown recruited 29 t-MDS patients and reported comparable results between de novo MDS and t-MDS patients, although there were no data to support this conclusion.36
MDS accrual in currently recruiting trials
Forty-nine trials had currently recruiting status until the year 2026. All of these trials were recruiting primary MDS patients (n = 22) or primary MDS, AML, or CMML patients (n = 27). When examining eligibility criteria, 10% (5 of 49) included t-MDS patients, whereas 10% excluded t-MDS patients. The reported accrual goal for trials exclusively studying primary MDS was 2987 MDS patients. The remaining trials studying MDS, AML, or CMML had an accrual goal of 5546 patients.
Clinical trial sponsors
Across the 128 published trials with t-MDS patient enrollment information, the proportion of trials including t-MDS patients was 14.5% (10 of 69) in pharmaceutical-sponsored trials, similar to the proportion of 13.6% (8 of 59) with nonpharmaceutical sponsors (P = 1.0). The results were similar when looking at the completed trials only, with 15.7% (8 of 51) categorized as pharmaceutical-sponsored trials and 13.2% (5 of 38) as nonpharmaceutical-sponsored trials (P = 1.000). When looking at the proportion of t-MDS (of all MDS patients) included across all published trials, there was a statistically significant difference between the pharmaceutical-sponsored trials (128 [2.8%] of 4573) and nonpharmaceutical-sponsored trials (103 [4.0%] of 2599; P = .0073), although the magnitude of the difference was small.
Discussion
t-MDS, defined as MDS with a history of exposure to chemotherapy and/or radiotherapy,3 is the most prevalent type of secondary MDS and falls under the WHO category of therapy-related neoplasms. Typically, t-MDS patients present with a higher number of chromosomal abnormalities associated with poor clinical outcomes and are categorized as high risk from patient and disease perspectives.1,4,5 Historically, MDS clinical trials have had strict eligibility criteria, with t-MDS patients less likely to be recruited.4,8
To understand how this has affected t-MDS patients, we analyzed therapeutic MDS clinical trials studying untreated MDS patients of any risk stratification, registered on ClinicalTrials.gov in the past 20 years. We quantified t-MDS accrual, significant findings regarding t-MDS patient outcomes, and factors influencing exclusion. We also estimated future t-MDS accrual based on currently recruiting clinical trials.
The proportion of t-MDS patients accrued was not consistent with estimated t-MDS prevalence in a newly diagnosed MDS population (10%-20%).1,4,,-7 In the 128 publications evaluated in this research, t-MDS patients accounted for one-third to one-sixth of the expected t-MDS patient population recruited and studied, a significantly smaller percentage than the estimated prevalence (P < .0001 when H0 = 10.0%). Therefore, real-world t-MDS patients are likely receiving therapies based on data from clinical trials in which they are underrepresented and may not be representative of their outcomes.
This low percentage of t-MDS accrual could have been due to a variety of reasons, the first, and most obvious, being the direct exclusion of t-MDS patients. A small percentage of published trials (14.8%) belonged to group A (trials directly excluding those with t-MDS), whereas 73% belonged to group B (trials not indicating exclusion or inclusion of t-MDS patients).
In general, group B trials excluded t-MDS and MDS patients based on arbitrary criteria, such as Eastern Cooperative Oncology Group performance score, organ function, and history of hepatitis or HIV, making it unlikely that these criteria were designed to exclude t-MDS specifically (Table 3). However, 29% of trials belonging to group B excluded patients with a previous malignancy within the past 1 to 5 years.22,26,37,,,,,,,,,,,-49 This likely excluded t-MDS patients from the trial patient population without directly saying so. In the same manner, all trials excluded patients with secondary t-MDS directly, without performing mutational analysis or clarifying that the exclusion of these patients was due to the complexity of their genetic profiles. It would be more effective if these trials had screened patients for mutations associated with poor outcomes instead of assuming patients with t-MDS had complex genetic profiles initially.
Several major oncology societies, including ASCO and the NCI, recently acknowledged this pattern of exclusion in clinical trials. The NCI recently released a document providing guidance for protocol development and trial designs that are more inclusive of patients with previous malignancies and preexisting conditions, such as HIV and hepatitis B or C, a promising first step toward including patients who represent the real-world experience.50
We also identified that the formal inclusion of t-MDS patients, using inclusive eligibility criteria, did not necessarily result in t-MDS recruitment, publications, or results. In group C (trials specifically including t-MDS patients), 11% (3 of 27) reported conclusions about t-MDS outcomes. Two of the studies that did accrue a large number of t-MDS patients reported similar outcomes for t-MDS patients who received previous radiotherapy only compared with de novo patients.35,36
Another factor that may have influenced t-MDS accrual was sponsorship type. Across all published trials, nonpharmaceutical-sponsored trials accrued a small but statistically higher percentage of t-MDS patients compared with trials sponsored by pharmaceutical companies (4.0% vs 2.8%; P = .0073). These findings suggest that nonpharmaceutical-sponsored trials seem to be more inclusive, but more investigation is needed to establish the validity of this finding.
Our study suggests that unless current eligibility criteria reflect real-world MDS patients, a significantly smaller proportion of newly diagnosed t-MDS patients will be represented in therapeutic MDS clinical trials within the next 8 years. Currently recruiting MDS trials have an accrual goal of 2987 patients. If we assume these trials meet the accrual goal, and t-MDS patients are underrepresented at the same proportion as the completed trials in our study (3.2%), then only 95 t-MDS patients will be enrolled in the next 8 years. There are ∼30 000 to 40 000 estimated new MDS cases per year, with 320 000 new cases of MDS predicted by 2026.51,52 Because t-MDS patients account for ∼10% to 20% of the total MDS population, we estimate there will be 32 000 to 64 000 new cases of t-MDS by the year 2026, which is highly disproportionate to their anticipated accrual.1,4,,-7
These results should be interpreted within the context of the following limitations. The data collection was done manually as opposed to using an automated algorithm. Our main source for identification of these studies was ClinicalTrials.gov, which is not always up to date. We adjusted for these limitations by basing most of our conclusions on t-MDS patient accrual from completed trials, with published manuscripts or abstracts.
We limited the scope of our research to phase 2 and 3 trials investigating first-line treatments. These typically have the highest likelihood of regulatory approval, with broader real-world MDS patient treatment applicability. We excluded phase 1 trials and trials studying relapsed/refractory MDS that may have included t-MDS patients, because these trials typically determine drug safety and tolerability and do not always advance to phase 2/3 studies.
In addition, we did not use the search term therapy-related AML, because we wanted to focus our study on patients with MDS only. It may be interesting to investigate the exclusion of therapy-related AML based on these results in t-MDS patients.
Finally, we used the 10% incidence of t-MDS among all MDS patients as our control proportion. Although the more relevant figure might be the proportion of t-MDS patients among the subgroup of all MDS patients eligible for trials, we cannot accurately estimate this number, because these patients are excluded from trials based on heterogeneous criteria. Therefore, we used the prevalence of secondary MDS as a comparator.
In conclusion, there are a significant number of completed and ongoing therapeutic MDS clinical trials excluding or failing to recruit t-MDS patients. We hope that our study, along with recent NCI/ASCO/American Society of Hematology guidelines for expanded eligibility criteria, can initiate meaningful change on how to approach high-risk MDS studies, reduce eligibility criteria bias, and design trials that are more inclusive, a critical step in improving prognostic models and treatment options for t-MDS patients in the future.
Presented in abstract form at the 59th annual meeting of the American Society of Hematology, Atlanta, GA, 9 December 2017.
Authorship
Contribution: U.B. designed the research; B.A.N. and T.B. performed data collection and created figures; R.F. performed statistical analysis of figures and data; and U.B., B.A.N., A.S., and M.A.S. wrote the paper.
Conflict-of-interest disclosure: U.B. is a consultant for Novartis and Jazz Pharmaceuticals. M.A.S. serves on the advisory committee for Celgene and on the advisory board for Takeda/Millennium Pharmaceuticals. The remaining authors declare no competing financial interests.
Correspondence: Uma Borate, Department of Hematology and Medical Oncology, Oregon Health and Science University, 3181 SW Sam Jackson Park Rd, Portland, OR 97239; e-mail: borate@ohsu.edu.

