

Key Points
Haploidentical BMT is potentially curative treatment option for the increasing population of patients age 70 and over with blood cancers.
NRM is associated with weight loss, and the causes of death are often those found in older patients without cancer.

Abstract
Hematologic malignancies in older people are unlikely to be cured with chemotherapy alone. Advances in allogeneic blood or marrow transplantation (alloBMT), especially nonmyeloablative (NMA) conditioning and the use of haploidentical donors, now make this therapy available to older people; however, long-term outcomes and predictors of success are unclear. We reviewed the outcomes of 93 consecutive patients aged 70 and older (median, 72; range, 70-78), who underwent haploidentical BMT at Johns Hopkins Hospital between 1 September 2009 and 1 April 2018. All patients received NMA conditioning and posttransplantation cyclophosphamide (PTCy) as graft-versus-host disease (GVHD) prophylaxis. The 2-year overall survival was 53%, and 2-year event-free survival was 43%. The 180-day cumulative incidence (CuI) of nonrelapse mortality (NRM) was 14%, and the 2-year CuI was 27%. The 2-year CuI of relapse was 30%. Of 78 patients who were alive and had their weight recorded on day 180, weight loss predicted subsequent NRM (subdistribution hazard ratio, 1.0; 95% CI, 1-1.13; P = .048). In conclusion, haploidentical BMT with PTCy is feasible and relatively safe in septuagenarians. Although early, 6-month NRM was relatively low at 14%, but overall NRM continued to climb to 27% at 2 years, at least in part because of late deaths that appeared to be somewhat age related. Further studies to elucidate predictors of NRM are warranted.
Introduction
The incidence of most hematologic malignancies rises with age, with a median age of onset in the seventh decade of life.1 Adverse biologic characteristics in these cancers also increase in prevalence with age.2 Even traditional markers of favorable-risk disease may not be favorable in an older patient.3 Thus, a large proportion of older patients with hematologic malignancies could benefit from allogeneic blood or marrow transplantation (alloBMT) to cure their illnesses. Older age historically has been considered a relative contraindication for alloBMT,4 as physicians are often concerned about excess nonrelapse mortality (NRM). NRM increases with myeloablative conditioning,5 worse performance status, poor scores on geriatric assessments,6 and a high level of comorbidity7 in older adults. Nevertheless, older patients with acute leukemia or aggressive lymphomas who achieve remission are increasingly receiving consolidation with alloBMT, as nonmyeloablative (NMA) conditioning,5,8 improved prevention and treatment of side effects, and risk-assessment tools have made transplantation feasible in older adults.9-12
Posttransplantation cyclophosphamide (PTCy) promotes engraftment of T-cell–replete allografts with acceptable rates of graft-versus-host disease (GVHD),13 thus expanding the available donor pool to include mismatched donors. This finding is particularly important for older patients whose older siblings may be less likely to be both available and healthy. Haploidentical children, as well as younger second-degree relatives, such as nieces, nephews, and even grandchildren,14 can now be used safely, especially for those patients lacking matched unrelated donor options. Although recent publications have reported on the experience of older adults undergoing haploidentical grafts with PTCy, none focused exclusively on the very old.15,16
Herein, we report the outcomes of patients aged 70 and older who underwent haploidentical BMT at Johns Hopkins Hospital (JHH) with PTCy-based GVHD prophylaxis.
Methods
We retrospectively evaluated all haploidentical patients age 70 or older who underwent alloBMT at JHH (Baltimore, MD) from 1 September 2009 through 1 April 2018. The study was conducted in accordance with the Declaration of Helsinki and with the approval of the JHH Institutional Review Board. Patient comorbidities were stratified according to the hematopoietic cell transplantation–comorbidity index (HCT-CI)17 and their disease according to the refined disease risk index (rDRI).18 All patients received NMA conditioning consisting of fludarabine 24 mg/m2 on days −6 through −2, cyclophosphamide 14.5 mg/kg on days −6 and −5, and 200 cGy total body irradiation. All patients received PTCy and mycophenolate mofetil from days 5 to 35 and either tacrolimus or sirolimus from day 5 until days 60 to 180.19 This report expands upon the report by Kasamon and colleagues,11 which included the first 27 of these patients aged ≥70 years.
Acute GVHD was staged according to the Keystone Criteria,20 and chronic GVHD was graded according to NIH Consensus Criteria.21 Neutrophil engraftment was defined as the first of 3 consecutive days with an absolute neutrophil count >0.5 × 109/L, and platelet engraftment the first of 3 days with platelets >20 × 109/L without a transfusion in the preceding 7 days. Eligibility criteria for NMA BMT typically included Eastern Cooperative Oncology Group (ECOG) performance status (PS) ≤2, left ventricular ejection fraction ≥35%, forced expiratory volume in 1 second and forced vital capacity ≥40% of predicted (≥60% of predicted after thoracic or mantle irradiation), and absence of uncontrolled infection. Morphologic complete remission of acute leukemia and at least partial remission of aggressive lymphoma were standard requirements.
Statistical methods
Overall survival (OS) was defined as the time from date of BMT to either death from any cause or until the last follow-up date for patients who are alive. Progression-free survival (PFS) was defined as the time from date of BMT to the time of relapse or death, whichever occurred first. Patients who neither relapsed nor died were treated as censored at the last follow-up date for PFS. NRM was a competing event for relapse, and relapse was a competing event for NRM when estimating the cumulative incidence (CuI) of relapse and NRM. Graft failure was a competing event for GVHD when estimating the CuI of GVHD. When applicable, 95% confidence intervals (CIs) were provided.
Baseline characteristics were descriptively summarized. Median follow-up was estimated via reverse Kaplan-Meier (KM) method.22 OS and PFS were summarized using the KM method with the Greenwood formula for variance. Cox proportional hazards models were used to assess the effects of baseline variables on OS/PFS. CuI of relapse, NRM, and GVHD were estimated with the competing events described in the prior paragraph.23 Subdistribution hazard regression (SDHR) models were used to assess the effects of baseline variables on relapse, NRM, and GVHD.24,25 For evaluating the effects of weight loss, landmark analysis was used, with the landmark time selected at day 180 after BMT. The landmark time was chosen for the following reasons: most patients had a weight measurement at this time point, and most patients would be expected to have recovered from most toxicities associated with conditioning chemotherapy and radiation. Multivariate analyses were conducted for assessing the association between clinical outcomes (OS/NRM) and weight loss, with the potential confounder adjustments selected based on clinical judgements and number of outcome events. All analyses were performed with statistical software R version 3.4.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patients
Ninety-five consecutive patients aged 70 and older underwent haploidentical alloBMT at JHH; 2 were excluded as having undergone a second allogeneic transplantation, leaving 93 evaluable cases. Their characteristics are listed in Table 1. The median age was 72, and 69% were male. The HCT-CI was ≥3 in 33% of patients, with a score of ≥5 in 9 patients.
Patient and donor demographics
| Characteristic | Data (N = 93) |
|---|---|
| Median patient age (range), y | 72 (70-78) |
| Male sex, n (%) | 64 (69) |
| Disease, n | |
| NHL | 33 |
| AML | 33 |
| MDS | 17 |
| MPN | 4 |
| CML, second CP | 2 |
| ALL | 2 |
| Other* | 2 |
| rDRI, n (%) | |
| Low | 8 (9) |
| Intermediate | 73 (78) |
| High/very high | 11 (12) |
| NA | 1 (1) |
| HCT-CI, n (%) | |
| 0 | 23 (25) |
| 1-2 | 38 (41) |
| ≥3 | 31 (33) |
| KPS, n (%) | |
| 70-80 | 23 (25) |
| 90 | 52 (56) |
| 100 | 18 (19) |
| Year of transplant, n (%) | |
| 2009-2014 | 39 (42) |
| 2015-2017 | 54 (58) |
| Median donor age (range), y | 43 (16-69) |
| Graft source, n (%) | |
| Bone marrow | 69 (74) |
| Peripheral blood | 24 (26) |
| CMV status, n (%) | |
| R−/D− | 36 (39) |
| R+/D- | 24 (26) |
| R−/D+ | 4 (4) |
| R+/D+ | 27 (29) |
| Missing | 2 (2) |
| Characteristic | Data (N = 93) |
|---|---|
| Median patient age (range), y | 72 (70-78) |
| Male sex, n (%) | 64 (69) |
| Disease, n | |
| NHL | 33 |
| AML | 33 |
| MDS | 17 |
| MPN | 4 |
| CML, second CP | 2 |
| ALL | 2 |
| Other* | 2 |
| rDRI, n (%) | |
| Low | 8 (9) |
| Intermediate | 73 (78) |
| High/very high | 11 (12) |
| NA | 1 (1) |
| HCT-CI, n (%) | |
| 0 | 23 (25) |
| 1-2 | 38 (41) |
| ≥3 | 31 (33) |
| KPS, n (%) | |
| 70-80 | 23 (25) |
| 90 | 52 (56) |
| 100 | 18 (19) |
| Year of transplant, n (%) | |
| 2009-2014 | 39 (42) |
| 2015-2017 | 54 (58) |
| Median donor age (range), y | 43 (16-69) |
| Graft source, n (%) | |
| Bone marrow | 69 (74) |
| Peripheral blood | 24 (26) |
| CMV status, n (%) | |
| R−/D− | 36 (39) |
| R+/D- | 24 (26) |
| R−/D+ | 4 (4) |
| R+/D+ | 27 (29) |
| Missing | 2 (2) |
ALL, acute lymphoblastic leukemia; CMV, cytomegalovirus; CML, chronic myelogenous leukemia; CP, chronic phase; D, donor; KPS, Karnofsky Performance Status; MPN, myeloproliferative neoplasm; NHL, non-Hodgkin lymphoma; R recipient.
Plasmacytoid dendritic cell neoplasm and multiple myeloma.
Donors were 4 siblings, 78 children, 7 grandchildren, and 4 nieces and nephews.14 Allografts were harvested from the BM in 74% of cases and from granulocyte colony–stimulating factor–stimulated peripheral blood (PB) in 26%. The decision to use BM or PB was based on the center’s guidelines at the time. Before 2015, all patients received BM grafts. Thereafter, diseases that were associated with higher rates of graft failure or relapse, such as myelodysplastic syndromes (MDSs), chronic lymphocytic leukemia (CLL), myeloproliferative disorders, and acute myeloid leukemia (AML), with minimal residual disease (MRD), were treated with PB grafts.
Outcomes
The median follow-up for the entire cohort was 33.4 months (range, 0.5-80.0), estimated using the reverse KM approach. The median time to neutrophil recovery was 18 days (range, 12-43), and the median time to platelet recovery was 27 days (range, 11-374). The CuI of graft failure was 7% (95% CI, 2%-12%) at 100 days and did not differ between BM (7.2%) and PB (8.3%) grafts (P = .86).
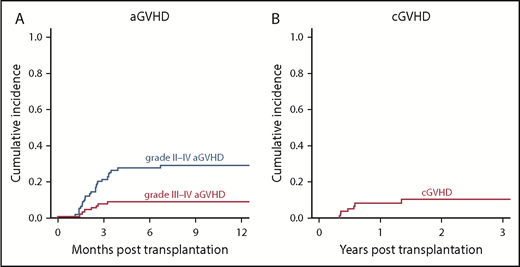
The estimated 1-year CuI of grade II to VI GVHD was 29% (95% CI, 19%-39%) and of grade III and IV GVHD was 9% (95% CI, 3%-19%; Figure 1A). The estimated 2-year CuI of chronic GVHD was 11% (95% CI, 3%-19%; Figure 1B). The median onset time for grade II to IV acute GVHD was 66 days (interquartile range [IQR], 48-87), 60 days (IQR, 47-77) for grade III and IV acute GVHD, and 189 days (IQR, 130-281) days for chronic GVHD. Compared with BM, PB allografts were not associated with an incidence in grade II to VI acute GVHD (23% with PB versus 31% with BM at 1 year; HR, 0.73; 95% CI, 0.28-1.94; P = .53) or chronic GVHD (6% with PB versus 9% with BM at 1 year; HR, 0.58; 95% CI, 0.07-4.56; P = .6).
The only significant predictor of relapse was donor age (Table 2; SDHR, 1.05 per 1 year older; 95% CI: 1.02-1.08; P < .001). Donor age did not predict OS (HR 1.02 per year; 95% CI 0.99-1.05; P = .24), in part perhaps because NRM was not influenced by donor age (SDHR, 0.99; 95% CI, 0.96-1.03; P = .66). The 180-day CuI of NRM was 14% (95% CI, 7%-21%), but 2-year NRM was 27% (95% CI, 18%-37%), with many late deaths. The causes of death are listed in Table 3. The association between HCT-CI and NRM was not statistically significant (SDHR, 0.66; [95% CI, 0.26-1.66; P = .38] for HCT-CI 1-2 vs 0; and SDHR, 0.76 [95% CI 0.29-1.99, P = .58] for HCT-CI, ≥3 vs 0).
Univariate analysis of factors on transplant outcomes
| NRM | Relapse | Event-free survival | OS | |||||
|---|---|---|---|---|---|---|---|---|
| Univariate | SDHR (95% CI) | P | SDHR (95% CI) | P | HR (95% CI) | P | HR (95% CI) | P |
| Patient age (per 1 y) | 1.17 (0.98-1.31) | .09 | 0.95 (0.80-1.12) | .53 | 1.08 (0.94-1.23) | .27 | 1.09 (0.94-1.26) | .24 |
| DRI | ||||||||
| Low | 0.35 (0.05-2.28) | .27 | 1.40 (0.38-5.09) | .61 | 0.78 (0.28-2.18) | .64 | 0.61 (0.19-1.97) | .41 |
| Intermediate | 1 | 1 | 1 | 1 | ||||
| High/very high | 0.27 (0.04-2.04) | .20 | 1.80 (0.67-4.87) | .24 | 0.96 (0.41-2.24) | .92 | 0.84 (0.33-2.14) | .71 |
| HCT-CI score | ||||||||
| 0 (low) | 1 | 1 | 1 | 1 | ||||
| 1-2 (intermediate) | 0.66 (0.26-1.66) | .38 | 1.35 (0.55-3.29) | .51 | 0.95 (0.50-1.83) | .88 | 0.70 (0.35-1.39) | .30 |
| ≥3 (high) | 0.76 (0.29-1.99) | .58 | 1.14 (0.45-2.91) | .78 | 0.93 (0.47-1.86) | .84 | 0.76 (0.37-1.55) | .45 |
| Donor age (per 1 y) | 0.99 (0.96-1.03) | .66 | 1.05 (1.02-1.08) | <.001 | 1.02 (0.99-1.05) | .11 | 1.02 (0.99 −1.05) | .24 |
| NRM | Relapse | Event-free survival | OS | |||||
|---|---|---|---|---|---|---|---|---|
| Univariate | SDHR (95% CI) | P | SDHR (95% CI) | P | HR (95% CI) | P | HR (95% CI) | P |
| Patient age (per 1 y) | 1.17 (0.98-1.31) | .09 | 0.95 (0.80-1.12) | .53 | 1.08 (0.94-1.23) | .27 | 1.09 (0.94-1.26) | .24 |
| DRI | ||||||||
| Low | 0.35 (0.05-2.28) | .27 | 1.40 (0.38-5.09) | .61 | 0.78 (0.28-2.18) | .64 | 0.61 (0.19-1.97) | .41 |
| Intermediate | 1 | 1 | 1 | 1 | ||||
| High/very high | 0.27 (0.04-2.04) | .20 | 1.80 (0.67-4.87) | .24 | 0.96 (0.41-2.24) | .92 | 0.84 (0.33-2.14) | .71 |
| HCT-CI score | ||||||||
| 0 (low) | 1 | 1 | 1 | 1 | ||||
| 1-2 (intermediate) | 0.66 (0.26-1.66) | .38 | 1.35 (0.55-3.29) | .51 | 0.95 (0.50-1.83) | .88 | 0.70 (0.35-1.39) | .30 |
| ≥3 (high) | 0.76 (0.29-1.99) | .58 | 1.14 (0.45-2.91) | .78 | 0.93 (0.47-1.86) | .84 | 0.76 (0.37-1.55) | .45 |
| Donor age (per 1 y) | 0.99 (0.96-1.03) | .66 | 1.05 (1.02-1.08) | <.001 | 1.02 (0.99-1.05) | .11 | 1.02 (0.99 −1.05) | .24 |
Causes and timing of NRM
| Causes of NRM (n = 25 total) | Days after transplantation |
|---|---|
| Infection (n = 11) | 14, 26, 76, 98, 111, 136, 146, 190, 299, 481, 543 |
| Cancer/cardiovascular disease (n = 5) | 107, 246, 426, 489, 1284 |
| Graft failure (n = 3) | 112, 512, 545 |
| GVHD (n = 2) | 66, 187 |
| Cytokine release syndrome (n = 2) | 21, 32 |
| Idiopathic pneumonia syndrome (n = 1) | 104 |
| Fall (n = 1) | 911 |
| Causes of NRM (n = 25 total) | Days after transplantation |
|---|---|
| Infection (n = 11) | 14, 26, 76, 98, 111, 136, 146, 190, 299, 481, 543 |
| Cancer/cardiovascular disease (n = 5) | 107, 246, 426, 489, 1284 |
| Graft failure (n = 3) | 112, 512, 545 |
| GVHD (n = 2) | 66, 187 |
| Cytokine release syndrome (n = 2) | 21, 32 |
| Idiopathic pneumonia syndrome (n = 1) | 104 |
| Fall (n = 1) | 911 |
PFS at 2 years was 43% (95% CI, 33%-56%). The OS of the entire cohort at 2 years was 53% (95% CI, 43%-65%; Figure 2). Table 2 shows univariate analyses. Patients aged 70 to 72 versus those aged 73 and older demonstrated a trend toward improved survival (median OS, 79.0 vs 17.4 months; HR, 1.7; P = .09). Year of transplantation (2015-2018 versus 2009-2014) did not significantly influence OS (median, 26.1 versus 31.4 months; HR, 1.02; 95% CI, 0.56-1.86; P = .94). rDRI was not significantly associated with OS (with intermediate as reference, HR for low, 0.61; 95% CI, 0.19 to 1.97; P = .41; HR for high/very high, 0.84; 95% CI, 0.33-2.14; P = .71), perhaps in part because of the low number of patients (n = 8) with low, high, or very high rDRI.

Outcomes of patients aged 70 and older who underwent allogeneic BMT. Kaplan-Meier curves of OS and PFS (A) and CuI of NRM and relapse (B).
Outcomes of patients aged 70 and older who underwent allogeneic BMT. Kaplan-Meier curves of OS and PFS (A) and CuI of NRM and relapse (B).
Weight loss and hospital stays
Given the high rate of later NRM, we performed an exploratory analysis of weight change, hospitalizations after transplantation, and NRM. Weight loss was chosen because it is associated with increased mortality in healthy older adults26,27 and in older patients with cancer,28 and it is a variable readily available in a retrospective chart review. For those who survived to day 180, median weight loss was 5.3% from initial admission weight. Absolute weight loss (median, 4.1 kg) and weight loss percentage correlated highly (Pearson correlation estimator, 0.97 (supplemental Figure 3A). A landmark analysis at 6 months (a date at which most patients had a weight recorded) demonstrated that weight loss was associated with OS (HR, 1.05 for each kilogram of weight change from baseline; 95% CI, 1-1.1; P = .032; Figure 3A). However, the relationship between weight loss and OS was less significant (HR, 1.04; 95% CI, 0.99-1.09; P = .083) after adjustment for age and rDRI. Weight loss predicted subsequent NRM (SDHR, 1.06, 95% CI 1-1.13; P = .04; Figure 3B) and retained significance when adjusted for age (SDHR, 1.07; 95% CI, 1.02-1.12; P = .008). Specifically, those who lost more than the median had a median OS of 36.9 months (95% CI, 17.8-NA) versus 79 months (95% CI, 32.3-NA) in the group that lost less than 4.1 kg (HR, 2.0; 95% CI, 0.89-4.5; P = .09). A similar result was obtained for weight loss percentage. There was no evidence that patients who experienced grade II to IV acute GVHD lost more weight (supplemental Figure 4; P = .82).
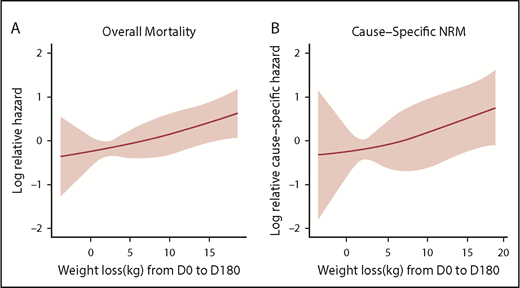
Mortality and weight loss. Hazard function of OS (A) and cause-specific hazard function of NRM (B) by weight loss (continuous per 1 kg). Three knots for weight loss, as a restricted cubic spline function, were selected based on the lowest Akaike Information Criteria.
Mortality and weight loss. Hazard function of OS (A) and cause-specific hazard function of NRM (B) by weight loss (continuous per 1 kg). Three knots for weight loss, as a restricted cubic spline function, were selected based on the lowest Akaike Information Criteria.
Hospitalizations in older patients are associated with a decrease in function.29-31 All reported patients were admitted from the start of conditioning through the recovery of neutrophils, given their advanced age. After achieving an absolute neutrophil count of 0.2 to 0.5 × 109/L, the patients were generally followed in our day hospital through day 60, and then seen weekly in our outpatient department through day 100, at which point their care was returned to their referring physicians. Patients were hospitalized for a median of 23 days between days 0 and 180, mostly during aplasia. Hospitalization for complications were associated with a poor outcome. For patients who were readmitted (n = 53), the median additional days spent in the hospital was 10 days (range, 1-114; IQR, 4-26). Patients who spent more than 10 days hospitalized after engraftment were less likely to survive (HR, 4.68; 95% CI, 1.64-13.33; P = .004; Figure 4A; Table 4) and more likely to suffer NRM (SDHR, 8.51; 95% CI, 1.8-40.22; P = .007; Figure 4B; Table 5) than those who were not hospitalized through day 180. Those who were hospitalized were also more likely to lose weight by day 180 (median weight loss of 3.0, 3.8, and 12.9 kg for those hospitalized 0, 1-10, and >10 days, respectively, P = .009, supplemental Figure 5). After adjustment for patient age and total days spent in the hospital, the coefficient estimates of weight loss on OS and NRM had only slight changes, although the effect was no longer statistically significant, which may have been caused by the loss of statistical power by adding covariates to a limited sample size.
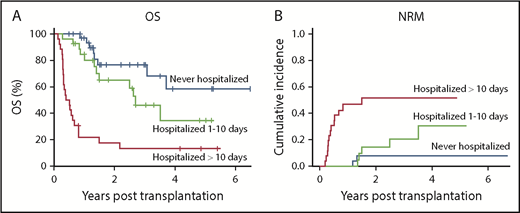
Association of hospitalization with survival. OS (A) and NRM (B) of patients aged 70 and older after haploidentical BMT according to days hospitalized between neutrophil recovery and day 180.
Association of hospitalization with survival. OS (A) and NRM (B) of patients aged 70 and older after haploidentical BMT according to days hospitalized between neutrophil recovery and day 180.
Univariate and multivariate results showing the associations of OS with weight loss and percentage weight loss
| Variables | Univariate HR (95% CI) | Multivariate HR (95% CI) | Variables | Univariate HR (95% CI) | Multivariate HR (95% CI) |
|---|---|---|---|---|---|
| Weight loss (per 1 kg) | 1.05 (1.00-1.10) P = .03 | 1.03 (0.98-1.08); P = .21 | % Weight loss (per 1%) | 1.04 (1.00-1.09); P = .06 | 1.02 (0.97-1.07); P = .40 |
| Age (per y) | 1.05 (0.83-1.33); P = .67 | Age (per y) | 1.06 (0.83-1.34); P = .66 | ||
| Hospital stay, d | Hospital stay, d | ||||
| 0 | 1 | 0 | 1 | ||
| 1-10 | 1.63 (0.58-4.58); P = .35 | 1-10 | 1.75 (0.64-4.82); P = .28 | ||
| >10 | 4.68 (1.64-13.33); P = .004 | >10 | 4.81 (1.64-14.08); P = .004 |
| Variables | Univariate HR (95% CI) | Multivariate HR (95% CI) | Variables | Univariate HR (95% CI) | Multivariate HR (95% CI) |
|---|---|---|---|---|---|
| Weight loss (per 1 kg) | 1.05 (1.00-1.10) P = .03 | 1.03 (0.98-1.08); P = .21 | % Weight loss (per 1%) | 1.04 (1.00-1.09); P = .06 | 1.02 (0.97-1.07); P = .40 |
| Age (per y) | 1.05 (0.83-1.33); P = .67 | Age (per y) | 1.06 (0.83-1.34); P = .66 | ||
| Hospital stay, d | Hospital stay, d | ||||
| 0 | 1 | 0 | 1 | ||
| 1-10 | 1.63 (0.58-4.58); P = .35 | 1-10 | 1.75 (0.64-4.82); P = .28 | ||
| >10 | 4.68 (1.64-13.33); P = .004 | >10 | 4.81 (1.64-14.08); P = .004 |
Univariate and multivariate results showing the associations of NRM with weight loss and percentage weight loss
| Variables | Univariate SDHR (95% CI) | Multivariate SDHR (95% CI) | Variables | Univariate SDHR (95% CI) | Multivariate SDHR (95% CI) |
|---|---|---|---|---|---|
| Weight loss (per 1 kg) | 1.06 (1.00-1.13); P = .04 | 1.05 (0.99-1.12); P = .11 | % Weight loss (per 1%) | 1.07 (1.00-1.15); P = .07 | 1.06 (0.99-1.13); P = .10 |
| Age (per y) | 1.55 (1.02-2.35); P = .04 | Age (per y) | 1.63 (1.05-2.54); P = .03 | ||
| Hospital stay, d | Hospital stay, d | ||||
| 0 | 1 | 0 | 1 | ||
| 1-10 | 1.81 (0.38-8.72); P = .46 | 1-10 | 1.81 (0.39-8.36); P = .45 | ||
| >10 | 8.51 (1.8-40.22); P = .007 | >10 | 7.6 (1.61-35.93); P = .01 |
| Variables | Univariate SDHR (95% CI) | Multivariate SDHR (95% CI) | Variables | Univariate SDHR (95% CI) | Multivariate SDHR (95% CI) |
|---|---|---|---|---|---|
| Weight loss (per 1 kg) | 1.06 (1.00-1.13); P = .04 | 1.05 (0.99-1.12); P = .11 | % Weight loss (per 1%) | 1.07 (1.00-1.15); P = .07 | 1.06 (0.99-1.13); P = .10 |
| Age (per y) | 1.55 (1.02-2.35); P = .04 | Age (per y) | 1.63 (1.05-2.54); P = .03 | ||
| Hospital stay, d | Hospital stay, d | ||||
| 0 | 1 | 0 | 1 | ||
| 1-10 | 1.81 (0.38-8.72); P = .46 | 1-10 | 1.81 (0.39-8.36); P = .45 | ||
| >10 | 8.51 (1.8-40.22); P = .007 | >10 | 7.6 (1.61-35.93); P = .01 |
Discussion
Septuagenarians with hematologic malignancies are often underserved by effective therapies because of worse disease biology and actual or perceived inability to tolerate the therapy.32,33 Long-term survival without alloBMT is unlikely with such diseases as AML and high-grade MDS.34 Our data suggest that haploidentical alloBMT is relatively safe and effective in this age group when NMA conditioning and PTCy are used. Rates of grades II to IV acute and chronic GVHD with PTCy are low and are similar to those in younger patients getting the same haploidentical alloBMT platform.35
Relapse continues to be a major cause of mortality. Relapse rates are lower when younger donors are used, although OS is not influenced. Younger donor age has been shown to be associated with higher OS in the setting of matched unrelated donor alloBMT,36 and younger donors are associated with superior outcomes after haploidentical transplantation, as well.16,37,38 The relationship between an aging immune system and decreased antitumor surveillance is well documented.39 How the hematopoietic compartment interacts with older host components, such as thymic40,41 and mesenchymal42 tissue is not known, although these interactions may be significant.41,43
Our oldest patients can still benefit from strategies to decrease NRM. Factors other than organ function (captured by the HCT-CI), such as geriatric assessments, are important in predicting who might be at risk for NRM after alloBMT.6,44-46 The upcoming Composite Health Assessment Risk Model (CHARM) study (clinicaltrials.gov BMT CTN 1704), which will include geriatric assessments in patients older than 60 who undergo alloBMT, may improve risk assessment in this growing population. In addition, efforts are underway at our institution to identify pretransplantation predictors of resilience in older patients who undergo alloBMT.
Recipient age in our cohort remained an important independent predictor of OS. Whereas early NRM was lower than many reports in older adults,12,47 non-GVHD NRM continued to climb beyond 2 years; in most studies of younger patients, non-GVHD NRM reaches a plateau at 1 year.13,48,49 Two-year NRM in our series is inferior to other reports of younger patients.50 Late deaths in our study were due to common conditions found in frail older adults, such as pneumonia, dementia, second cancers, and sequelae from falls. In an older group of patients, classic transplantation-related causes of death are only part of the problem, with persistent transplantation-related morbidity likely to make older cancer survivors vulnerable to subsequent health stressors. Transplantation may even accelerate some aspects of aging, such as neurocognitive decline.51
Weight loss during transplantation is associated with late mortality in this older group. Interventions targeted at promoting weight maintenance may reduce late mortality, if causal, and should be studied in an effort to reduce late mortality. Days spent in the hospital were also associated with increased mortality, likely reflecting the complications managed with hospitalization.
AlloBMT is being considered and offered with increasing frequency to older patients. As therapies aimed at controlling diseases before BMT are becoming more effective and better tolerated, it is likely that alloBMT could play even a larger role, since most of these therapies are unlikely to be curative. Classic alloBMT-associated complications such as early infection, GVHD, and relapse do not appear to be substantially higher in patients aged 70 or older. A prospective study in patients over the age of 50 identified several factors associated with increased NRM, including high C-reactive protein.6 Our results with haploidentical alloBMT appear at least comparable to a recent Center for International Blood and Marrow Transplant Research registry analysis of primarily matched donor alloBMT, in which septuagenarians who underwent transplantation between 2008 and 2013 had 33% NRM and 39% OS at 2 years.9 A large, single-center study in patients aged older than 70 demonstrated similar outcomes (OS at 2 years 39%) using matched or one locus (7 out of 8) mismatched donors.52 The favorable outcomes in our study may be related to lower HCT-CI scores in our cohort, or lower rates of GHVD associated with PTCy.53 Many studies now show that PTCy, despite its low associated incidence of GVHD, is not associated with higher relapse rates, regardless of graft type or conditioning intensity.53-56
Limitations of this analysis include its retrospective nature, the heterogeneity of underlying malignancy, and the relatively small sample size. Older patients referred for alloBMT are typically more fit as a group than others with hematologic malignancy, and applicability to the larger population with hematologic malignancy may be limited. Potential predictors of outcomes require further study. Nevertheless, this is the largest experience with haploidentical BMT in patients aged 70 and older and adds to an earlier publication that demonstrated the feasibility of the approach.11 Thus, septuagenarians with hematologic malignancies should not be arbitrarily excluded from alloBMT and should be counseled about its risks and benefits. Efforts to improve supportive care in these patients are warranted.
Presented in part at the Transplantation and Cellular Therapy Meetings, Houston, TX, 20-24 February 2019.
The full-text version of this article contains a data supplement.
Acknowledgments
This work was supported by National Institutes of Health grants UH2 AG056933 from the National Institute on Aging and P01 CA015396 from the National Cancer Institute.
Authorship
Contribution: P.H.I., R.V., and R.J.J. designed the study; L.L., E.J.F., C.A.H., D.E.G., R.F.A., I.M.B., L.J.S., N.W.-J., C.B.G., S.A.A., F.J.B.-M., and R.J.J. cared for patients; P.H.I., H.-L.T., P.L., R.V., and R.J.J. collected and analyzed the data; P.H.I., H.-L.T., R.V., and R.J.J. wrote the manuscript; and D.E.G. and F.J.B.-M. reviewed the manuscript.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Philip H. Imus, Division of Hematologic Malignancy, Johns Hopkins/Sidney Kimmel Comprehensive Cancer Center, 1650 Orleans St, CRB1 Room 2M10, Baltimore, MD 21217; e-mail: pimus1@jhmi.edu.

