

Key Points
Bortezomib combined with ICE/R is feasible and active in HIV+ lymphomas with evidence of gammaherpesvirus lytic activation as hypothesized.
Bortezomib induced an increase in the anti-HIV cytidine deaminase APOBEC3G.

Abstract
HIV-associated lymphomas (HALs) have high rates of latent infection by gammaherpesviruses (GHVs). We hypothesized that proteasome inhibition would induce lytic activation of GHVs and inhibit HIV infectivity via preservation of cytidine deaminase APOBEC3G, improving lymphoma control. We tested this oncolytic and antiviral strategy by using bortezomib combined with ifosfamide, carboplatin, and etoposide (ICE) alone or with rituximab (ICE/R) in relapsed/refractory HAL. A 3+3 dose-escalation design was used with a 7-day lead-in period of single-agent bortezomib. Bortezomib was administered intravenously on days 1 and 8 of each cycle at 1 of 4 dose levels: 0.7, 1.0, 1.3, or 1.5 mg/m2. ICE began day 8 of cycle 1 and day 1 of subsequent cycles. Rituximab was included on day 1 of cycles 2 to 6 for CD20+ lymphomas. Twenty-three patients were enrolled. The maximum tolerated dose of bortezomib was not reached. Grade 4 toxicities attributable to bortezomib were limited to myelosuppression. Responses occurred in 17 (77%) of 22 patients receiving any protocol therapy. The 1-year overall survival was 57%. After bortezomib alone, both patients with Kaposi sarcoma herpesvirus (KSHV)–positive lymphoma had more than a 1-log increase in KSHV viral load. In 12 patients with Epstein-Barr virus (EBV)–positive lymphoma, median values of EBV viral load increased. Undetectable HIV viremia at baseline in the majority of patients limited evaluation of HIV inhibition. APOBEC3G levels increased in 75% of evaluable patients. Bortezomib combined with ICE/R in patients with relapsed/refractory HAL is feasible with response and survival comparing favorably against previously reported second-line therapies. Changes in GHV viral loads and APOBEC3G levels trended as hypothesized. This trial was registered at www.clinicaltrials.gov as #NCT00598169.
Introduction
In persons living with HIV/AIDS, lymphomas occur at a much higher rate than in the HIV-seronegative population and represent the most common form of malignancy, accounting for nearly 25% of cancer cases.1,2 In contrast to most lymphomas in the HIV-seronegative population, HIV-associated lymphomas (HALs) are more commonly associated with gammaherpesviruses (GHVs) such as Epstein-Barr virus (EBV) and Kaposi sarcoma herpesvirus (KSHV), also known as human herpesvirus 8.3,4
Although survival has improved in recent years since the introduction of highly active antiretroviral therapy (ART), relapsed and refractory disease occurs in more than one-third of aggressive AIDS-associated non-Hodgkin5,6 and Hodgkin7 lymphomas. Some cases have been successfully managed with autologous hematopoietic stem cell transplantation (AHSCT)8 ; however, many patients with HAL are unable to achieve an adequate response to standard second-line lymphoma therapy that would allow them to proceed to AHSCT.9
Bortezomib (Velcade; Millennium Pharmaceuticals, Inc, Cambridge, MA) has activity in various types of non-Hodgkin lymphoma attributed at least in part to inhibition of nuclear factor κB.10,11 As a proteasome inhibitor, bortezomib may have additional mechanisms of action in HAL, such as induction of lytic activation of latent viral infections, including EBV and KSHV. Bortezomib was identified as the most potent lytic activator of EBV among ∼2500 US Food and Drug Administration–approved therapeutic agents screened.12 Lytic activation of the latent GHV infecting HIV lymphoma cells may result in direct cytotoxicity, as well as increased immune recognition of lymphoma, as lytic viral proteins promote immunogenicity. Furthermore, GHVs inhibit tumor suppressors, such as von Hippel-Lindau and p53, via ubiquitination,13 suggesting that bortezomib may restore tumor suppressor function.
In preclinical models, proteasome inhibition also reduced HIV infectivity through restoration of the cytidine deaminase APOBEC3G, an innate human defense against retroviruses.14 Human APOBEC3G is incorporated into nascent retroviral virions as they bud from an infected cell. This deaminase then enters the cell newly infected by a virion, resulting in hypermutation of the viral complementary DNA transcribed from the provirus, impairing faithful viral replication. HIV overcomes this antiviral pathway by using one of its accessory gene products, virion infectivity factor, to circumvent the APOBEC3G-mediated human defense mechanism. Virion infectivity factor induces ubiquitination of APOBEC3G, thereby targeting this protective host protein for proteasomal degradation, shortening the intracellular half-life of APOBEC3G.15 Thus, proteasome inhibition could potentially preserve APOBEC3G and help to restore resistance to HIV replication.
The primary objectives of the current phase 1 clinical trial (AIDS Malignancy Consortium [AMC]–053) were to evaluate the safety and overall response rate (ORR) of relapsed/refractory HAL to bortezomib combined with ifosfamide, carboplatin, and etoposide (ICE) chemotherapy, with the addition of rituximab (ICE/R) in patients with CD20+ disease. The secondary objectives included: estimating the impact of bortezomib on lytic activation of EBV and KSHV by using peripheral blood mononuclear cell (PBMC) viral loads, as well as on plasma HIV viral loads with a single copy assay and on the level of APOBEC3G in PBMC; to report overall survival at 1 year (1y-OS); and to correlate changes in EBV and KSHV viral load with lymphoma response.
Patients and methods
Protocol design and therapy
A 3+3 dose-escalation design assessed 4 levels of IV bortezomib in combination with ICE/R on days 1 and 8 of each cycle: 0.7 (cohort 1), 1.0 (cohort 2), 1.3 (cohort 3), or 1.5 (cohort 4) mg/m2. Cycle 1 was designed with a 7-day lead-in period of bortezomib alone, before bortezomib + ICE, to allow for assessment of early effects of bortezomib on APOBEC3G, as well as HIV, EBV, and KSHV viral loads. Combination chemotherapy with ICE, at standard doses (as detailed in the supplemental Methods),16 began day 8 of cycle 1 (28-day cycle) and day 1 of subsequent cycles (21-day cycle). For CD20+ lymphomas, rituximab dosed at 375 mg/m2 was administered on day 1 of cycles 2 to 6. Patients with central nervous system involvement or features suggesting a high risk of central nervous system involvement received intrathecal chemotherapy according to standard practice at the institution of the treating investigator. Required supportive care included granulocyte colony–stimulating factor and prophylaxis against Pneumocystis jirovecii, gram-negative bacteria, and herpes zoster. ART was continued during protocol therapy unless patients had not been receiving ART before enrollment, in which case it was not initiated until completion of protocol therapy. The dose-limiting toxicity (DLT) determination period spanned 7 weeks through cycle 2, day 21. The protocol strongly encouraged consideration of consolidation of responsive disease with AHSCT after ≥2 cycles of protocol therapy. Alternatively, patients were allowed to continue for 2 cycles beyond attaining a complete remission for a maximum of 6 cycles. Patients with progressive disease after ≥1 cycle or lack of at least a partial response (PR) by cycle 4 were not eligible for additional protocol treatment.
Key eligibility criteria
Inclusion criteria consisted of confirmation of HIV seropositivity and relapsed/refractory Hodgkin lymphoma or non-Hodgkin lymphoma with pathologic demonstration of GHV (either EBV or KSHV) infection within the lymphoma. Patients with non-germinal center (GC) diffuse large B-cell lymphoma (DLBCL) were also eligible regardless of GHV status based on evidence of constitutive activation of the nuclear factor κB transcription complex in this subtype.17 Patients undergoing ART at screening were required to have been on the same ART regimen for at least 12 weeks before enrollment. Other key eligibility requirements included: age ≥18 years, Eastern Cooperative Oncology Group Performance Status 0 to 2, absolute neutrophil count ≥1 × 109/L, hemoglobin level ≥8 g/dL, platelet level ≥100 × 109/L (unless cytopenias were attributed to marrow involvement), aspartate aminotransferase/alanine aminotransferase levels ≤2.5× upper limit of normal, and creatinine clearance levels ≥50 mL/min/1.73 m2. Individuals were excluded if they had poorly controlled comorbidities. However, patients with opportunistic infections or hepatitis B viral infection controlled by suppressive therapy were eligible. Additional exclusion criteria at the time of enrollment included pregnancy or breastfeeding, grade 2 or higher peripheral neuropathy, myocardial infarction or class III or higher congestive heart failure within the previous 6 months, persons requiring moderate or strong cytochrome P450 3A4 inhibitors other than HIV protease inhibitors, or previous treatment with the ICE chemotherapy regimen. Institutional review boards at each of the study sites approved the study protocol. This study was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent before treatment.
Measurements, monitoring, and assays
Local institutional pathology review of biopsy specimens from either the initial lymphoma presentation or time of relapse/refractory disease was used to confirm EBV, KSHV, or GC status for purposes of eligibility determination. KSHV presence was assessed by immunohistochemistry for latency-associated nuclear antigen; EBV presence was assessed by EBV-encoded RNA in situ hybridization or latent membrane protein 1 expression by immunohistochemistry. Hans criteria18 were used for immunohistochemistry determination of DLBCL GC status.
Adverse event monitoring was performed at all clinic and hospital visits. Severity was graded by using the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0.
Assessment of lymphoma response was performed before combination protocol therapy on day 8 of cycle 1 according to physical examination and after cycles 2, 4, and 6 according to 2007 Cheson criteria.19 Computed tomography (CT) scans of the chest, abdomen, and pelvis (as well as neck, if indicated) were required at these time points, whereas positron emission tomography (PET) or PET/CT imaging was strongly recommended at baseline and 4 to 6 weeks after completion of protocol therapy when possible. Bone marrow aspirate and biopsy and diagnostic lumbar puncture were required at baseline; they were required to be repeated for patients with initial involvement or signs/symptoms of new involvement in the respective site. The protocol did not define a minimum duration of response to meet criteria for PR or complete response (CR). Patients with a CR underwent physical examination and radiographic assessments every 3 months for 1 year unless receiving additional lymphoma therapy. The Functional Assessment of Cancer Therapy/Gynecologic Oncology Group–Neurotoxicity questionnaire20 was administered at baseline; cycle 1, day 8; at the start of each subsequent cycle; and following the conclusion of protocol therapy.
Blood samples to assess plasma HIV and PBMC EBV and/or KSHV viral loads and APOBEC3G levels were collected as follows: at baseline; during cycle 1 on days 2, 4, and 8 to evaluate effects of single-agent bortezomib; and on day 1 of each subsequent cycle. Plasma HIV viral load was determined by using real-time quantitative polymerase chain reaction, as previously described.21 Likewise, quantitative polymerase chain reaction was used to assay PBMC for KSHV and EBV viral loads (supplemental Methods). The amount of APOBEC3G in PBMC was determined by using western blot analysis.
Statistical analysis
Binomial proportions were used to estimate ORR. The product-limit (Kaplan-Meier) method was used to estimate 1y-OS. The Wilcoxon signed rank test was used to evaluate changes in viral loads and APOBEC3G levels.
Results
Twenty-three patients were enrolled from 7 sites within the AMC: 6, 8, 3, and 6 patients were enrolled into dose cohorts 1, 2, 3, and 4, respectively. As shown in Table 1, the median age was 48 years (range, 34-66 years), and >90% of enrolled patients were men. At baseline, 20 (87%) of the 23 patients were receiving ART; the median CD4+ count was 315 cells/μL (range, 45-773 cells/μL), and the median HIV viral load was undetectable (range, undetectable-241 490 copies/mL). More than one-half of patients had stage IV HAL. The majority (n = 15) had DLBCL, 9 of whom were EBV positive (2 of whom were also non-GC DLBCL subtype), 4 were EBV negative, and EBV status was not reported in 2 patients. Of the remaining patients, 2 had primary effusion lymphoma (PEL), 3 had plasmablastic lymphoma, and 2 had Hodgkin lymphoma.
Demographic and baseline characteristics
| Characteristic | n | % |
|---|---|---|
| Sex | ||
| Male | 20 | 91 |
| Female | 2 | 9 |
| Race | ||
| White | 15 | 68 |
| African American | 6 | 27 |
| Other | 1 | 5 |
| Ethnicity | ||
| Hispanic | 5 | 23 |
| Non-Hispanic | 17 | 77 |
| Age, y | ||
| Median | 48 | |
| Range | 34-66 | |
| CDC risk group | ||
| Homosexual/bisexual contact | 15 | 68 |
| Heterosexual contact | 5 | 23 |
| Homosexual and heterosexual contact | 1 | 5 |
| IV drug use | 1 | 5 |
| Receiving ART at enrollment | 20 | 87 |
| Absolute CD4 count, μL | ||
| Median | 315 | |
| Minimum-maximum | 45-773 | |
| HIV viral load, copies/mL | ||
| Median | Undetectable | |
| Minimum-maximum | Undetectable to 241 490 | |
| Ann Arbor stage | ||
| I | 3 | 14 |
| II | 3 | 14 |
| IIE | 1 | 5 |
| III | 3 | 14 |
| IV | 12 | 55 |
| Lymphoma diagnosis | ||
| DLBCL | 15 | 68 |
| PEL | 2 | 9 |
| Plasmablastic lymphoma | 3 | 14 |
| Hodgkin lymphoma | 2 | 9 |
| Characteristic | n | % |
|---|---|---|
| Sex | ||
| Male | 20 | 91 |
| Female | 2 | 9 |
| Race | ||
| White | 15 | 68 |
| African American | 6 | 27 |
| Other | 1 | 5 |
| Ethnicity | ||
| Hispanic | 5 | 23 |
| Non-Hispanic | 17 | 77 |
| Age, y | ||
| Median | 48 | |
| Range | 34-66 | |
| CDC risk group | ||
| Homosexual/bisexual contact | 15 | 68 |
| Heterosexual contact | 5 | 23 |
| Homosexual and heterosexual contact | 1 | 5 |
| IV drug use | 1 | 5 |
| Receiving ART at enrollment | 20 | 87 |
| Absolute CD4 count, μL | ||
| Median | 315 | |
| Minimum-maximum | 45-773 | |
| HIV viral load, copies/mL | ||
| Median | Undetectable | |
| Minimum-maximum | Undetectable to 241 490 | |
| Ann Arbor stage | ||
| I | 3 | 14 |
| II | 3 | 14 |
| IIE | 1 | 5 |
| III | 3 | 14 |
| IV | 12 | 55 |
| Lymphoma diagnosis | ||
| DLBCL | 15 | 68 |
| PEL | 2 | 9 |
| Plasmablastic lymphoma | 3 | 14 |
| Hodgkin lymphoma | 2 | 9 |
CDC, Centers for Disease Control and Prevention.
Two patients in dose cohort 2 (bortezomib 1.0 mg/m2) were not evaluable for DLT assessments, and thus the cohort was expanded to ensure 6 DLT-evaluable patients (8 total). One patient withdrew from the study before initiating treatment. The other patient withdrew after only receiving day 1 of protocol therapy (bortezomib alone). A third patient in cohort 2 completed <2 cycles due to complications of lymphomatous bowel involvement. Thus, of the 23 total patients, 20 completed ≥2 cycles of protocol therapy; 16 (70%) patients completed ≥3 cycles. Three patients terminated protocol treatment due to disease progression. Two patients terminated protocol treatment because of adverse events: in 1 case, grade 3 hypokalemia, hypophosphatemia, and neutropenia after cycle 2; in the other, the adverse events were assessed as not attributable to the single dose of bortezomib received.
The maximum tolerated dose of bortezomib was not reached at the highest dose cohort studied (1.5 mg/m2). DLTs occurred in 2 patients in cohort 1, each consisting of uncomplicated grade 4 cytopenias expected for ICE chemotherapy alone, after which the protocol was amended to redefine hematologic DLTs as febrile neutropenia (absolute neutrophil count <0.5 × 109/L) requiring critical care (pressor support or intubation) or severe thrombocytopenia (platelet levels <25 × 109/L) resulting in life-threatening bleeding or treatment delay for >2 weeks. Under the amended criteria, a single DLT (grade 3 febrile neutropenia) occurred in cohort 2, and no DLTs occurred in cohorts 3 and 4. Treatment delays and/or dose reductions occurred in 2 of 20, 4 of 18, 2 of 12, and 4 of 24 cycles in dosing cohorts 1, 2, 3, and 4, respectively. Forty-two serious adverse events were reported in 11 patients, with 20 attributed as at least possibly related to bortezomib (Table 2). All adverse events are listed in supplemental Tables 1 and 2. Mean and median Functional Assessment of Cancer Therapy/Gynecologic Oncology Group–Neurotoxicity scores did not exhibit significant change over the course of the study (supplemental Table 3).
Adverse events assessed as at least possibly related to bortezomib
| CTC system organ class | CTC adverse event term | CTC adverse event grade | All | |||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| N | N | N | N | N | ||
| Blood and lymphatic system disorders | Anemia | 0 | 5 | 9 | 0 | 14 |
| Febrile neutropenia | 0 | 0 | 2 | 0 | 2 | |
| Eye disorders | Blurred vision | 1 | 0 | 0 | 0 | 1 |
| Gastrointestinal disorders | Abdominal pain | 0 | 0 | 1 | 0 | 1 |
| Constipation | 1 | 1 | 0 | 0 | 2 | |
| Diarrhea | 1 | 1 | 2 | 0 | 4 | |
| Mucositis oral | 1 | 1 | 0 | 0 | 2 | |
| Nausea | 4 | 0 | 0 | 0 | 4 | |
| Vomiting | 3 | 0 | 0 | 0 | 3 | |
| General disorders and administration site conditions | Fatigue | 4 | 0 | 1 | 0 | 5 |
| Fever | 1 | 0 | 0 | 0 | 1 | |
| Injection site reaction | 1 | 0 | 0 | 0 | 1 | |
| Pain | 1 | 0 | 0 | 0 | 1 | |
| Infections and infestations | Mucosal infection | 1 | 0 | 0 | 0 | 1 |
| Investigations | Alkaline phosphatase increase | 2 | 0 | 0 | 0 | 2 |
| Lymphocyte count decreased | 1 | 0 | 3 | 2 | 6 | |
| Neutrophil count decreased | 0 | 2 | 2 | 8 | 12 | |
| Platelet count decreased | 0 | 1 | 4 | 7 | 12 | |
| White blood cell decreased | 0 | 2 | 1 | 7 | 10 | |
| Metabolism and nutrition disorders | Anorexia | 1 | 1 | 0 | 0 | 2 |
| Hypokalemia | 0 | 0 | 1 | 0 | 1 | |
| Hypomagnesemia | 1 | 0 | 0 | 0 | 1 | |
| Hyponatremia | 1 | 0 | 0 | 0 | 1 | |
| Hypophosphatemia | 0 | 1 | 4 | 0 | 5 | |
| Nervous system disorders | Dysgeusia | 1 | 0 | 0 | 0 | 1 |
| Headache | 2 | 1 | 0 | 0 | 3 | |
| Neuralgia | 1 | 0 | 1 | 0 | 2 | |
| Paresthesia | 1 | 0 | 0 | 0 | 1 | |
| Peripheral sensory neuropathy | 2 | 0 | 0 | 0 | 2 | |
| Seizure | 0 | 0 | 1 | 0 | 1 | |
| Syncope | 0 | 0 | 1 | 0 | 1 | |
| Psychiatric disorders | Insomnia | 0 | 1 | 0 | 0 | 1 |
| Respiratory disorders | Cough | 1 | 0 | 0 | 0 | 1 |
| Skin and subcutaneous tissue disorders | Alopecia | 0 | 1 | 0 | 0 | 1 |
| Vascular disorders | Hypotension | 0 | 0 | 2 | 0 | 2 |
| CTC system organ class | CTC adverse event term | CTC adverse event grade | All | |||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| N | N | N | N | N | ||
| Blood and lymphatic system disorders | Anemia | 0 | 5 | 9 | 0 | 14 |
| Febrile neutropenia | 0 | 0 | 2 | 0 | 2 | |
| Eye disorders | Blurred vision | 1 | 0 | 0 | 0 | 1 |
| Gastrointestinal disorders | Abdominal pain | 0 | 0 | 1 | 0 | 1 |
| Constipation | 1 | 1 | 0 | 0 | 2 | |
| Diarrhea | 1 | 1 | 2 | 0 | 4 | |
| Mucositis oral | 1 | 1 | 0 | 0 | 2 | |
| Nausea | 4 | 0 | 0 | 0 | 4 | |
| Vomiting | 3 | 0 | 0 | 0 | 3 | |
| General disorders and administration site conditions | Fatigue | 4 | 0 | 1 | 0 | 5 |
| Fever | 1 | 0 | 0 | 0 | 1 | |
| Injection site reaction | 1 | 0 | 0 | 0 | 1 | |
| Pain | 1 | 0 | 0 | 0 | 1 | |
| Infections and infestations | Mucosal infection | 1 | 0 | 0 | 0 | 1 |
| Investigations | Alkaline phosphatase increase | 2 | 0 | 0 | 0 | 2 |
| Lymphocyte count decreased | 1 | 0 | 3 | 2 | 6 | |
| Neutrophil count decreased | 0 | 2 | 2 | 8 | 12 | |
| Platelet count decreased | 0 | 1 | 4 | 7 | 12 | |
| White blood cell decreased | 0 | 2 | 1 | 7 | 10 | |
| Metabolism and nutrition disorders | Anorexia | 1 | 1 | 0 | 0 | 2 |
| Hypokalemia | 0 | 0 | 1 | 0 | 1 | |
| Hypomagnesemia | 1 | 0 | 0 | 0 | 1 | |
| Hyponatremia | 1 | 0 | 0 | 0 | 1 | |
| Hypophosphatemia | 0 | 1 | 4 | 0 | 5 | |
| Nervous system disorders | Dysgeusia | 1 | 0 | 0 | 0 | 1 |
| Headache | 2 | 1 | 0 | 0 | 3 | |
| Neuralgia | 1 | 0 | 1 | 0 | 2 | |
| Paresthesia | 1 | 0 | 0 | 0 | 1 | |
| Peripheral sensory neuropathy | 2 | 0 | 0 | 0 | 2 | |
| Seizure | 0 | 0 | 1 | 0 | 1 | |
| Syncope | 0 | 0 | 1 | 0 | 1 | |
| Psychiatric disorders | Insomnia | 0 | 1 | 0 | 0 | 1 |
| Respiratory disorders | Cough | 1 | 0 | 0 | 0 | 1 |
| Skin and subcutaneous tissue disorders | Alopecia | 0 | 1 | 0 | 0 | 1 |
| Vascular disorders | Hypotension | 0 | 0 | 2 | 0 | 2 |
CTC, Common Toxicity Criteria.
Responses occurred in 17 of the 22 patients initiating protocol therapy. PET or PET/CT imaging was incorporated into baseline staging in 6 patients and response assessment in 12 patients; CT and magnetic resonance imaging were used in the remainder for radiographic assessment of response. There were 7 CRs and 10 PRs for an ORR of 77% in those receiving any protocol therapy. Median duration of response was >40 weeks (range, 2 to >67 weeks), with all but 5 patients still in response at last follow-up. Of the 20 patients who completed ≥2 cycles, the ORR was 85% (95% confidence interval, 62-97), and 1y-OS was 57% (95% confidence interval, 30-77). Response and survival according to lymphoma histologic subtype were as follows: DLBCL, 11 of 13 receiving at least 2 cycles responded (4 CRs), 8 of 13 alive at last follow-up; plasmablastic, 2 of 3 responded (1 CR), 2 of 3 alive at last follow-up; PEL, 2 of 2 responded (1 CR), 1 of 2 alive at last follow-up; and Hodgkin lymphoma, 2 of 2 responded (1 CR) and 2 of 2 alive at last follow-up. Of the six patients without a response, one did not receive any protocol therapy, one did not complete cycle 1, one did not complete cycle 2, and two of the remaining three were treated at the lowest dose level of bortezomib. There was a trend toward increased response and 1-year overall survival rates with increased bortezomib dose. One patient with EBV- and KSHV-positive PEL, refractory to upfront therapy with dose-adjusted etoposide, doxorubicin, vincristine, cyclophosphamide, and prednisone (EPOCH), was noted to have a 50% decrease in the size of palpable lymphadenopathy and a 30% decrease in the size of pleural effusion after administration of bortezomib alone. Eight of 9 deaths occurring during the study were attributable to disease progression. One patient died of sepsis and Legionella attributed to complications of AHSCT after completion of protocol therapy. Nine patients (3 CRs, 5 PRs, and 1 stable disease) underwent AHSCT, with 6 of 9 alive at last follow-up. Details on each patient are summarized in Table 3.
Patient-specific disease characteristics, treatment, and outcome
| Lymphoma type | Ann Arbor stage | Lymphoma EBV/KSHV status | Baseline CD4, cells/μL | Baseline HIV, copies/mL | Bortezomib dose cohort, mg/m2 | Total no. of cycles completed | Best response | Duration of response, wk | Postprotocol lymphoma therapy | Survival, wk |
|---|---|---|---|---|---|---|---|---|---|---|
| DLBCL | IV | EBV positive | 294 | 241 490 | 0.7 | 6 | CR | >68.5 | None | >68 |
| DLBCL | IV | EBV positive | 77 | 85 122 | 0.7 | 2 | PD* | NA | Radiation | 38 |
| DLBCL | IV | EBV positive | 402 | 170 | 0.7 | 4 | CR* | >55 | None | >55 |
| Plasmablastic | IV | EBV positive | 169 | 126 | 0.7 | 2 | SD | NA | AHSCT | 29 |
| PEL | IV | EBV and KSHV positive | 570 | 48 | 0.7 | 4 | PR | 15 | AHSCT | 24 |
| DLBCL | II | EBV positive | 261 | — | 0.7 | 2 | PD | NA | Radiation | 26 |
| DLBCL | IV | EBV positive | 336 | Undetectable | 1.0 | 3 | PR* | 4 | Not reported | 19 |
| Not reported | — | — | — | — | 1.0 | 0 | NA | NA | NA | NA |
| DLBCL | IV | EBV positive | 48 | 8000 | 1.0 | <2 | NE | NE | Not reported | 9 |
| DLBCL | IV | EBV positive | 45 | 89 | 1.0 | <1 | NE | NE | None | 3 |
| Hodgkin | III | EBV positive | 283 | <400 | 1.0 | 2 | CR* | >55 | AHSCT | >55 |
| Plasmablastic | I | EBV positive | 476 | <20 | 1.0 | 4 | CR* | >59 | AHSCT | >59 |
| DLBCL | IIE | EBV positive | 435 | Undetectable | 1.0 | 3 | PR | >40 | AHSCT | >40 |
| DLBCL | IV | EBV negative | 334 | 4.4 | 1.0 | 3 | PR* | 6 | Not reported | >13 |
| Hodgkin | III | EBV positive | 356 | 0.7 | 1.3 | 3 | PR | >60 | AHSCT | >60 |
| PEL | II | EBV and KSHV positive | 450 | 1.2 | 1.3 | 6 | CR* | >58 | None | >58 |
| DLBCL | III | EBV negative | 237 | 0.4 | 1.3 | 3 | PR | >55 | AHSCT | >55 |
| Plasmablastic | I | EBV positive | 294 | 0.45 | 1.5 | 4 | PR | 5 | Not reported | >14 |
| DLBCL | IV | EBV negative | 296 | 24 817 | 1.5 | 3 | CR* | >43 | None | 52 |
| DLBCL | IV | EBV positive | 401 | 24 | 1.5 | 5 | PR* | >65 | Radiation | >65 |
| DLBCL | I | Unknown | 241 | 4.2 | 1.5 | 3 | PR | 2 | Not reported | >12 |
| DLBCL | II | Unknown | 773 | 1.3 | 1.5 | 4 | PR* | >52 | R2-GemOx + AHSCT | >52 |
| DLBCL | IV | EBV negative | 339 | Undetectable | 1.5 | 3 | CR* | 6† | AHSCT | 16 |
| Lymphoma type | Ann Arbor stage | Lymphoma EBV/KSHV status | Baseline CD4, cells/μL | Baseline HIV, copies/mL | Bortezomib dose cohort, mg/m2 | Total no. of cycles completed | Best response | Duration of response, wk | Postprotocol lymphoma therapy | Survival, wk |
|---|---|---|---|---|---|---|---|---|---|---|
| DLBCL | IV | EBV positive | 294 | 241 490 | 0.7 | 6 | CR | >68.5 | None | >68 |
| DLBCL | IV | EBV positive | 77 | 85 122 | 0.7 | 2 | PD* | NA | Radiation | 38 |
| DLBCL | IV | EBV positive | 402 | 170 | 0.7 | 4 | CR* | >55 | None | >55 |
| Plasmablastic | IV | EBV positive | 169 | 126 | 0.7 | 2 | SD | NA | AHSCT | 29 |
| PEL | IV | EBV and KSHV positive | 570 | 48 | 0.7 | 4 | PR | 15 | AHSCT | 24 |
| DLBCL | II | EBV positive | 261 | — | 0.7 | 2 | PD | NA | Radiation | 26 |
| DLBCL | IV | EBV positive | 336 | Undetectable | 1.0 | 3 | PR* | 4 | Not reported | 19 |
| Not reported | — | — | — | — | 1.0 | 0 | NA | NA | NA | NA |
| DLBCL | IV | EBV positive | 48 | 8000 | 1.0 | <2 | NE | NE | Not reported | 9 |
| DLBCL | IV | EBV positive | 45 | 89 | 1.0 | <1 | NE | NE | None | 3 |
| Hodgkin | III | EBV positive | 283 | <400 | 1.0 | 2 | CR* | >55 | AHSCT | >55 |
| Plasmablastic | I | EBV positive | 476 | <20 | 1.0 | 4 | CR* | >59 | AHSCT | >59 |
| DLBCL | IIE | EBV positive | 435 | Undetectable | 1.0 | 3 | PR | >40 | AHSCT | >40 |
| DLBCL | IV | EBV negative | 334 | 4.4 | 1.0 | 3 | PR* | 6 | Not reported | >13 |
| Hodgkin | III | EBV positive | 356 | 0.7 | 1.3 | 3 | PR | >60 | AHSCT | >60 |
| PEL | II | EBV and KSHV positive | 450 | 1.2 | 1.3 | 6 | CR* | >58 | None | >58 |
| DLBCL | III | EBV negative | 237 | 0.4 | 1.3 | 3 | PR | >55 | AHSCT | >55 |
| Plasmablastic | I | EBV positive | 294 | 0.45 | 1.5 | 4 | PR | 5 | Not reported | >14 |
| DLBCL | IV | EBV negative | 296 | 24 817 | 1.5 | 3 | CR* | >43 | None | 52 |
| DLBCL | IV | EBV positive | 401 | 24 | 1.5 | 5 | PR* | >65 | Radiation | >65 |
| DLBCL | I | Unknown | 241 | 4.2 | 1.5 | 3 | PR | 2 | Not reported | >12 |
| DLBCL | II | Unknown | 773 | 1.3 | 1.5 | 4 | PR* | >52 | R2-GemOx + AHSCT | >52 |
| DLBCL | IV | EBV negative | 339 | Undetectable | 1.5 | 3 | CR* | 6† | AHSCT | 16 |
NA, not applicable; NE, not evaluable; PD, progressive disease; R2-GemOx, lenalidomide, rituximab, gemcitabine, and oxaliplatin; SD, stable disease.
PET imaging used in response assessment.
In continued CR at time of death attributed to complications of AHSCT.
In patients with GHV-positive lymphomas, EBV and/or KSHV PBMC viral loads were evaluated for change after treatment with bortezomib alone, as an indication of lytic activation. In patients with EBV-positive lymphomas, median values of EBV PBMC viral load revealed a nonstatistically significant increase from baseline to day 8 of 1224 to 1650 copies/106 PBMC (n = 12; P = .770). Paired analysis did not identify a statistically significant change in this small sample (n = 12), and there was no correlation found between change in EBV viral load and response. The 2 patients with known KSHV-positive PEL each had more than a 1-log increase in day 8 KSHV viral load compared with baseline (Figure 1). Both patients with PEL achieved a response from protocol therapy (1 CR). No patient developed adverse events attributable to lytic activation of EBV or KSHV.
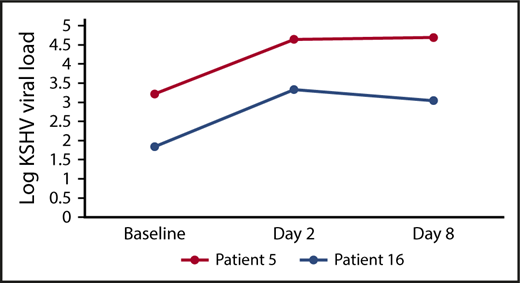
PBMC KSHV viral load change in patients with PEL. More than 1 log-increase occurred in PBMC KSHV viral load after bortezomib administration in the 2 patients with KSHV-positive PEL, both of whom achieved a response to protocol therapy (1 CR, 1 PR).
PBMC KSHV viral load change in patients with PEL. More than 1 log-increase occurred in PBMC KSHV viral load after bortezomib administration in the 2 patients with KSHV-positive PEL, both of whom achieved a response to protocol therapy (1 CR, 1 PR).
HIV viral loads were assessable at both baseline and during the first cycle in 14 patients. Eight patients had <5 copies of HIV per milliliter of plasma at baseline on single copy testing (range, 0.4-4.4 copies/mL). In these 8 patients, none had >4 copies/mL absolute increase or decrease noted within the first 2 weeks. The remaining 6 patients had detectable baseline HIV viremia according to standard clinical or single copy viral load assays. By day 8, three of these six patients had a decrease in HIV viral load by 0.2, 0.5, and 0.5 log, respectively; one patient had no significant change (decrease of 0.04 log); and two patients had an increase in HIV viral load by 0.2 and 2 log. Two of 3 patients not receiving ART at protocol entry experienced decreased HIV viral load by day 8 of protocol therapy after administration of single-agent bortezomib (Figure 2).
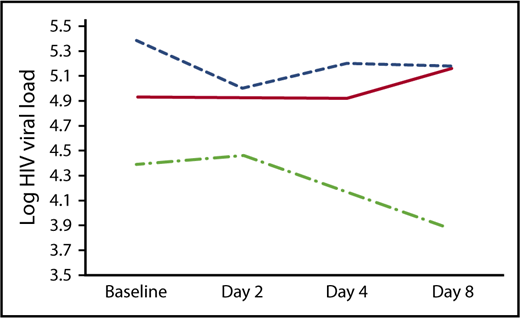
Plasma HIV viral load change in patients not receiving ART. Three patients not already undergoing ART at enrollment did not start ART until completion of protocol therapy. Plasma HIV viral load data during cycle 1 are plotted here for each patient, demonstrating a downward trend as hypothesized in 2 of the 3 patients throughout the first week of protocol therapy, during which patients received single-agent bortezomib.
Plasma HIV viral load change in patients not receiving ART. Three patients not already undergoing ART at enrollment did not start ART until completion of protocol therapy. Plasma HIV viral load data during cycle 1 are plotted here for each patient, demonstrating a downward trend as hypothesized in 2 of the 3 patients throughout the first week of protocol therapy, during which patients received single-agent bortezomib.
APOBEC3G was evaluable at both pretreatment baseline and during the first week after single-agent bortezomib administration in 12 patients. APOBEC3G levels increased in 9 of the 12 patients (Figure 3). The median fold change in APOBEC3G after bortezomib administration was 1.2 (P = .15). No correlation was found between change in APOBEC3G levels and bortezomib dose, baseline plasma HIV viral load, or change in HIV viral load. The latter assessment was particularly limited, with only 7 patients having evaluable data for HIV and APOBEC3G at both time points.
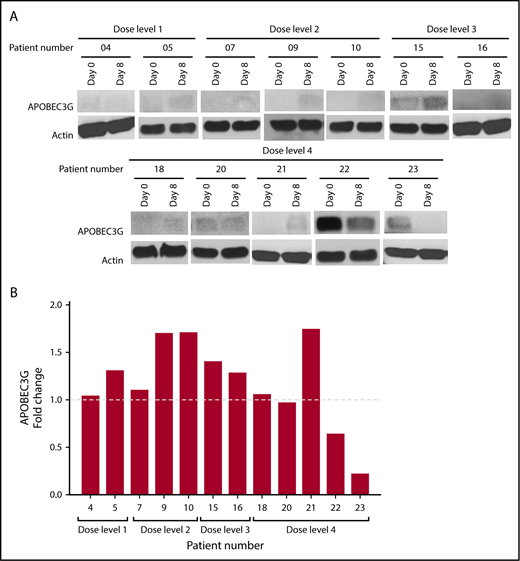
APOBEC3G levels increased in 75% of evaluable patients after bortezomib administration. APOBEC3G was measured by using western blot on PBMC from 12 patients. (A) PBMCs from both baseline and day 8 were lysed, and proteins were separated by using sodium dodecyl sulfate/polyacrylamide gel electrophoresis. Gel lanes were reordered in the figure to group according to bortezomib dose level. (B) APOBEC3G level was quantified by using ImageJ software (National Institutes of Health, Bethesda, MD), and the results are presented as a fold change in the level of APOBEC3G normalized to actin.
APOBEC3G levels increased in 75% of evaluable patients after bortezomib administration. APOBEC3G was measured by using western blot on PBMC from 12 patients. (A) PBMCs from both baseline and day 8 were lysed, and proteins were separated by using sodium dodecyl sulfate/polyacrylamide gel electrophoresis. Gel lanes were reordered in the figure to group according to bortezomib dose level. (B) APOBEC3G level was quantified by using ImageJ software (National Institutes of Health, Bethesda, MD), and the results are presented as a fold change in the level of APOBEC3G normalized to actin.
Discussion
In this dose-finding safety and efficacy study, addition of bortezomib to ICE/R in relapsed/refractory HAL was feasible and tolerable. Treatment delays and dose reductions were infrequent. Because neurotoxicity is an expected side effect of bortezomib, the ICE regimen, and certain ARV agents, as well as a possible complication of HIV infection, neurotoxicity was carefully monitored. Neurotoxicity was not found to be a limiting adverse event of this bortezomib-containing protocol therapy. However, because patients with baseline peripheral neuropathy of grade 2 or greater were excluded from this study, we cannot recommend use of the regimen in this context. Because IV administration of bortezomib was standard of care at the time of this protocol’s inception, subcutaneous administration was not used. Subcutaneous administration of bortezomib, when combined with ICE/R, would be expected to further reduce the risk of neuropathy.22
Although the current study lacked a comparator arm, the ORR (77%) and 1y-OS (57%) compare favorably against other published second-line therapies for HAL,23,24 including an AMC retrospective review of relapsed/refractory HAL that reported an ORR of 37% and 1y-OS of 41% (n = 88). This study also reported outcomes of a subset of non-Hodgkin lymphoma treated with ICE/R (including DLBCL and other non-Hodgkin lymphoma histologies) having an ORR of 32% and 1y-OS of 38% (n = 31).9 In our study, best response and OS rates at last follow-up were at least 50% in each of the tested subtypes of HAL, including PEL and plasmablastic lymphoma, the latter of which is known to have poor prognosis.25,26 A recently reported retrospective study of bortezomib combined with dose-adjusted EPOCH as upfront therapy similarly noted higher-than-expected response and survival rates in 6 cases of HIV-associated plasmablastic lymphoma.27 Of note in the current study, lymphoma regression was observed in 1 patient with PEL after single-agent bortezomib administration, demonstrating activity of proteasome inhibition in this difficult-to-treat HAL subtype. Within our study, there was also a trend toward increased response and 1y-OS with increased bortezomib dose, further supporting the hypothesis that bortezomib adds to the activity of ICE/R. The current trial also showed that consolidation of response to bortezomib plus ICE/R with AHSCT was feasible in HAL, consistent with a previous study using bortezomib with ICE in the HIV-seronegative Hodgkin lymphoma population.28
Response duration was durable in the majority of patients. As expected, depth of responses was associated with durability, as none of the 7 patients with CR experienced disease progression at last follow-up (median, 55 weeks) despite only 3 patients receiving consolidation with AHSCT. In contrast, responses were short-lived in 5 of 10 patients initially meeting criteria for PR. Four of these progressions occurred within 6 weeks (range, 2-6 weeks; 3 DLBCL, 1 plasmablastic lymphoma), before the opportunity to consolidate with AHSCT. An additional patient with PEL, who underwent consolidation of PR with AHSCT, progressed at week 15, dying of lymphoma progression 12 weeks after completing protocol therapy. The remaining 5 patients with PR all received consolidation with either AHSCT (n = 4) or radiation (n = 1) and were alive in continued response at last follow-up (median, 55 weeks).
Determination of effects of proteasome inhibition on EBV, KSHV, HIV, and APOBEC3G were inherently limited by the dose-finding nature of this study. However, the data suggest that GHV lytic activation occurs with bortezomib alone, as hypothesized. No consistent pattern of effect on HIV was apparent; however, the majority of baseline HIV viral loads were <5 copies/mL, which limited assessment of any suppressive effect of bortezomib on HIV replication. Consistent with previous in vitro data showing recovery of APOBEC3G in HIV-infected cells after proteasome inhibition,15 levels of this cytidine deaminase increased after bortezomib administration in 75% of evaluable patients, supporting a potential antiretroviral effect of bortezomib in humans.
In conclusion, bortezomib combined with ICE/R was feasible and active in all tested subtypes of relapsed/refractory HAL, with response and survival comparing favorably against previously reported second-line therapies. In addition, the data suggest that bortezomib affects GHV lytic activation. Notably, to the best of our knowledge, this analysis is the first in-human study to report the effects of proteasome inhibition on APOBEC3G, showing levels of this anti-HIV cytidine deaminase increased in the majority of evaluable subjects after bortezomib treatment. Based on the favorable clinical outcomes observed, the effect on APOBEC3G, and the impact on GHV lytic activation, additional study of bortezomib and other proteasome inhibitors in HAL and GHV-positive lymphoma is warranted.
Preliminary results presented in abstract form at the 58th annual meeting of the American Society of Hematology, San Diego, CA, 5 December 2016.
The full-text version of this article contains a data supplement.
Acknowledgments
The authors gratefully acknowledge the participating patients and their caregivers, as well as all AMC subinvestigators and research staff contributing to the conduct of this protocol.
This study was supported by a National Institutes of Health (NIH), National Cancer Institute U01 AMC grant (UM1CA121947), the NIH Bench to Bedside Award (3U01CA121947-03S2) (E.R. and F.M.), NIH Cancer Center Support Grant: UCSD Cancer Clinical Investigator Team Leadership Award (E.R.) and Mentored Translational Research Award (P30CA023100) (E.R. and W.W.), and a Millennium Pharmaceuticals unrestricted grant for investigator-initiated trial support to the University of California, San Diego (X05199).
Authorship
Contribution: E.G.R., as protocol chair, designed and oversaw conduct of the protocol, assisted in data analysis, and prepared the manuscript; W.W., as protocol co-chair, contributed to protocol design, conduct, and manuscript preparation. D.A., R.A., D.H., R.M., A.N., J.C.R., and J.S. performed additional trial conduct and manuscript preparation; R.A., E.C., D.L., F.M., and S.Y. performed correlative studies and also contributed to manuscript preparation; and J.L. performed statistical analysis and contributed to manuscript preparation.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
A complete list of the members of the AIDS Malignancy Consortium appears in the supplemental appendix.
Correspondence: Erin G. Reid, University of California, San Diego, Moores Cancer Center, 3855 Health Sciences Dr, MC 0987, La Jolla, CA 92093-0987; e-mail: egreid@ucsd.edu.

