

Key Points
Patients with D30 PR/SD with subsequent conversion to CR experience similar early outcomes as patients who achieved CR by D30.
SUVmax ≥ 10 may help to identify patients with D30 PR/SD who are at risk for subsequent progression.
Abstract
About 70% of patients with large B-cell lymphoma (LBCL) who are treated with axicabtagene ciloleucel (axi-cel) and who achieve a partial response (PR) or stable disease (SD) on the day 30 (D30) positron emission tomography (PET)–computed tomography (CT) scan progress; however, the factors that are predictive of progression are unknown. This a retrospective study of patients with LBCL who were treated with axi-cel at MD Anderson Cancer Center between January of 2018 and February of 2021. Among 50 patients with D30 PR/SD, 13 (26%) converted to a complete response (CR). Among 95 patients with a D30 CR, 72 (76%) remained in CR. On univariate analysis, the only day −5 characteristic associated with conversion from D30 PR/SD to subsequent CR was a higher platelet count (P = .05). The only D30 factor associated with conversion from D30 PR/SD to subsequent CR was a lower maximum standardized uptake volume (SUVmax; P < .001); all patients with D30 SUVmax ≥ 10 progressed. After a median follow-up of 12 months, no significant difference in median progression-free survival was observed between patients who converted from D30 PR/SD to subsequent CR and those who had been in CR since D30 (P = .19). Novel predictive and prognostic markers based on tissue biopsy and noninvasive diagnostic assays are needed to more effectively identify these patients and characterize the biology of their residual disease.
Introduction
Approximately 40% of patients with relapsed or refractory large B-cell lymphoma (LBCL) treated with chimeric antigen receptor (CAR) T-cell therapy will achieve a durable remission, with similar rates reported across all 3 products approved by the US Food and Drug Administration.1-4 Patients who are refractory to CAR T-cell therapy, detected with early clinical or radiological progression observed on day 30 (D30) positron emission tomography (PET)–computed tomography (CT) scan, experience very poor outcomes, with an estimated survival <6 months.5 In addition, 70% of patients who achieve a partial response (PR) or stable disease (SD) on D30 PET-CT scan will eventually have disease progression and experience equally poor outcomes.6 Therefore, a deeper clinical and biological characterization of these patients with D30 PR is necessary to help identify those at risk for progression and to develop optimal consolidation strategies.
Methods
This is a single-center retrospective study of all patients with relapsed and/or refractory LBCL achieving PR or SD on D30 PET-CT scan after receiving standard-of-care axicabtagene ciloleucel (axi-cel) at MD Anderson Cancer Center between January of 2018 and February of 2021; the data cutoff was April of 2021. The study was approved by the MD Anderson Cancer Center Institutional Review Board and conducted in accordance with institutional guidelines and the principles of the Declaration of Helsinki.
The clinical characteristics and laboratory features before lymphodepleting chemotherapy (day −5) and at the time of first PET-CT scan restaging (D30) were confirmed by review of the medical records. Response status was determined using the Lugano 2014 classification.7 Maximum standardized uptake volume (SUVmax) was calculated as previously described, and lesions suspicious for alternative etiologies were excluded from the analysis.8 The receiver operating characteristic method was used to identify optimal SUVmax thresholds.
The association between categorical variables was evaluated using the χ2 test or Fisher’s exact test. The difference in a continuous variable between patient groups was evaluated by the Mann-Whitney test. Progression-free survival (PFS) was defined as the time from axi-cel to progression of disease, death, or last follow-up (whichever occurred first). Overall survival (OS) was defined as the time from axi-cel infusion to death or last follow-up. PFS and OS were calculated using Kaplan-Meier estimates and compared using the log-rank test. A P value ≤ .05 (2-tailed) was considered statistically significant. Statistical analyses were performed using SPSS 24 and GraphPad Prism 8.
Results and discussion
On D30, 204 of 206 treated patients were evaluable for response, and 2 were lost to follow-up. Among the 204 evaluable patients, 102 (50%) achieved complete response (CR), 49 (24%) achieved PR, 8 (4%) achieved SD, and 45 (22%) experienced clinical or radiological progressive disease (PD). Among the 57 patients who achieved PR/SD on the D30 PET-CT scan, 50 were evaluable for response at D90 or beyond and were included in the final analysis, 5 were lost to follow-up, and 2 died of unrelated cause before restaging. Among the 50 evaluable patients with D30 PR/SD, 13 (26%) converted to CR on subsequent restaging without additional therapy, and 37 (74%) had PD. Among the 102 patients with D30 CR, 7 were lost to follow-up. In the remaining 95 evaluable patients, 72 (76%) remained in CR at day 90 restaging, and 13 (24%) progressed (Figure 1A).
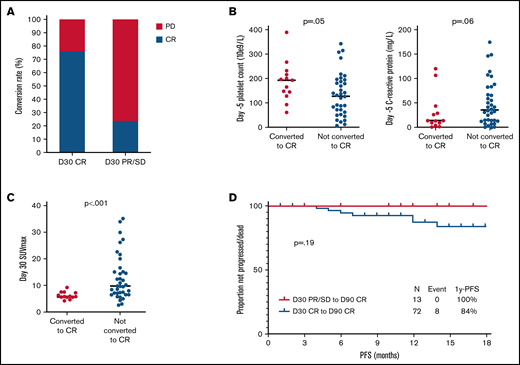
Factors associated with conversion of D30 PR/SD to subsequent CR. (A) Rates of conversion to CR among patients with D30 CR and D30 PR/SD. (B) Baseline characteristics associated with conversion of D30 PR/SD to D90 CR. (C) Association between D30 SUVmax and conversion of D30 PR/SD to D90 CR. (D) PFS among patients converting from D30 PR to CR compared with those achieving D30 CR. None of the patients who converted from D30 PR/SD to subsequent CR experienced progression. All patients with D30 PR and SUVmax ≥ 10 progressed.
Factors associated with conversion of D30 PR/SD to subsequent CR. (A) Rates of conversion to CR among patients with D30 CR and D30 PR/SD. (B) Baseline characteristics associated with conversion of D30 PR/SD to D90 CR. (C) Association between D30 SUVmax and conversion of D30 PR/SD to D90 CR. (D) PFS among patients converting from D30 PR to CR compared with those achieving D30 CR. None of the patients who converted from D30 PR/SD to subsequent CR experienced progression. All patients with D30 PR and SUVmax ≥ 10 progressed.
Baseline characteristics (on day −5) are shown in Table 1. On univariate analysis, the only baseline characteristic associated with conversion from D30 PR/SD to subsequent CR was a higher platelet count (median, 193 × 109/L vs 128 × 109/L; P = .05), as a surrogate marker for bone marrow reserve; a trend for an association with lower C-reactive protein was also observed (13.7 mg/L vs 36 mg/L; P = .06) (Figure 1B; supplemental Table 1). No difference in baseline characteristics was observed when comparing patients in CR at D30 with those with PR at D30 who subsequently converted to CR (supplemental Table 2).
Laboratory, clinical, and radiological characteristics collected on D30 are shown in Table 1. On univariate analysis, the only D30 factor associated with conversion from D30 PR/SD to subsequent CR was lower D30 SUVmax (median, 5.8 vs 9.8; P < .001) (supplemental Table 3). At D30, 8 of 14 (57%) patients with SUVmax < 6 eventually converted to CR, in contrast with patients with SUVmax ≥ 6, of whom 5 of 36 (14%) converted to CR. All patients with D30 SUVmax ≥ 10 had subsequent PD (Figure 1C); this was identified as the optimal threshold (sensitivity, 100%; specificity, 52%).
After a median follow-up of 12 months (95% confidence interval, 11-13), no significant difference in median PFS was observed when comparing the 13 patients with D30 PR/SD and subsequent CR with the 72 patients with D30 CR (1-year PFS rate, 100% vs 84%; P = .19) (Figure 1D). Furthermore, no significant difference in median PFS was observed in a landmark analysis at 90 days (P = .19).
PR/SD on D30 PET-CT scan, defined by a Deauville score of 4 to 5, can present with a variable range of fluorodeoxyglucose avidity, commonly summarized by SUVmax. Other PET-based parameters relevant to patients with active disease include tumor burden, measured as total metabolic tumor volume (TMTV), and the combination of fluorodeoxyglucose avidity and tumor burden, measured as total lesion glycolysis (TLG). SUVmax, TMTV, and TLG have shown prognostic and predictive value in patients with LBCL and among those treated with CAR T-cell therapy, as also shown in this study.9-12 Although the availability of TMTV and TLG remains limited, SUVmax is commonly and easily calculated and may be of significant value in the management of patients with D30 PR/SD. Further investigation of the clinical utility of early intervention among patients treated with CAR T-cell therapy is warranted.
Along with radiological parameters, other noninvasive techniques are being developed to identify high-risk patients. For example, detection of circulating tumor DNA within the first 30 days of CAR T-cell therapy may allow for early identification of patients who will develop refractory disease; if still detectable at D30, it is associated with poor outcomes.13,14
Although the approaches outlined above may help to identify patients with D30 PR/SD who are at risk for progression, the optimal consolidation strategy for these patients remains unknown. Limited data are available regarding the use of third-line US Food and Drug Administration–approved agents for patients with LBCL after CAR T-cell therapy. In this patient population, response rates of 42% and 44% were reported with the use of loncastuximab tesirine and polatuzumab vedotin, respectively.15,16 There are no data regarding the efficacy of other third-line agents, such as tafasitamab and selinexor, in this setting.17,18 Other promising potential consolidations strategies have been reported with the off-label use of agents that enhance CAR T-cell activity and favorably impact the host tumor immune environment, including ibrutinib, lenalidomide, pembrolizumab, and radiation therapy.13,19-24
We acknowledge multiple limitations of this study, including its small sample size, its single-center and retrospective nature, and the lack of central review for SUVmax measurements and of more objective measurements, such as TMTV and TLG.
In conclusion, patients with D30 PR/SD who subsequently convert to CR experience similar favorable outcomes as patients who achieve CR by D30. PET-associated parameters, such as SUVmax ≥ 10, may help to identify patients with D30 PR/SD who are at risk for subsequent progression and who may benefit from clinical trials of consolidation therapy. Novel predictive and prognostic markers based on tissue biopsy for patients with D30 PR/SD, as well as noninvasive diagnostic assays, are needed to more effectively identify these patients and characterize the biology of their residual disease.
Acknowledgments
This work was supported in part by The University of Texas M.D. Anderson Cancer Center Support Grant from the National Institutes of Health National Cancer Institute (P30 CA016672). P.S. is supported by a Lymphoma Research Foundation Career Development Award and by the R21 National Institutes of Health grant.
Authorship
Contribution: A.A.Z. analyzed data and wrote the manuscript; J.R.W., S.A.A., L.J.N., M.H., R.N., S.P.I., H.J.L., R.S., C.R.F., E.J.S., P.K., and S.S.N. provided clinical care to patients and coauthored the paper; G.W. and H.M. collected clinical data and coauthored the paper; L.F. provided statistical support and coauthored the paper; and P.S. designed the study, analyzed data, provided clinical care to patients, and wrote the manuscript.
Conflict-of-interest disclosure: P.S. has served a consultant for Roche-Genentech, Hutchison MediPharma, ADC Therapeutics and TG Therapeutics and has received research funds from Astra Zeneca-Acerta and ALX Oncology. R.S. has received research funding from Seagen, Bristol Myers Squibb, Rafael Pharmaceuticals, and GlaxoSmithKline. S.A.A. has received research funding from Seattle Genetics, Merck, Xencor, and Tessa Therapeutics and is on the advisory committee for Tessa Therapeutics. L.J.N. has received honoraria from Celgene, Genentech, Gilead, Janssen, Juno, Novartis, Spectrum, and TG Therapeutics and research support from Celgene, Genentech, Janssen, Karus Therapeutics, and Merck. S.S.N. has served as a consultant for Kite, a Gilead Company, Merck, Bristol Myers Squibb, Novartis, Celgene, Pfizer, Allogene Therapeutics, Cell Medica/Kuur, Incyte, Precision Biosciences, Legend Biotech, Adicet Bio, Calibr, and Unum Therapeutics; has received research support from Kite, a Gilead Company, Bristol Myers Squibb, Merck, Poseida, Cellectis, Celgene, Karus Therapeutics, Unum Therapeutics, Allogene Therapeutics, Precision Biosciences, and Acerta; has received royalties from Takeda Pharmaceuticals; and has intellectual property related to cell therapy. The remaining authors declare no competing financial interests.
Correspondence: Paolo Strati, Department of Lymphoma and Myeloma, Department of Translational Molecular Pathology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Unit 429, Houston, TX 77030; e-mail: pstrati@mdanderson.org.



