Key Points
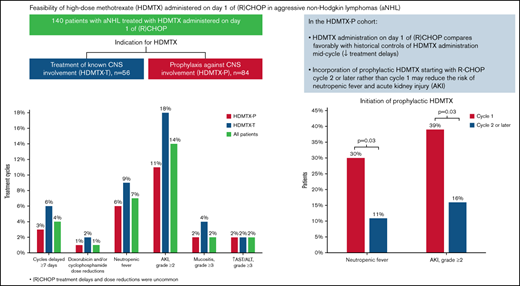
HDMTX administration on day 1 of (R)CHOP is feasible and compares favorably with reports of HDMTX administration midcycle.
Delaying prophylactic HDMTX beyond cycle 1 of (R)CHOP might lower the risks of neutropenic fever and acute kidney injury.

Abstract
The optimal timing for administering high-dose methotrexate (HDMTX) when combined with (R)CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone, with/without rituximab) is unclear. Recent data showed that the administration of prophylactic HDMTX before day 10 of R- CHOP may lead to fewer treatment delays. Herein, we report our experience with HDMTX administered on day 1 of (R)CHOP in patients with aggressive non-Hodgkin lymphoma (NHL). We identified 140 patients treated with ≥1 cycle of HDMTX combined with (R)CHOP for prophylaxis against (n = 84) or treatment of (n = 56) central nervous system (CNS) involvement. Overall, (R)CHOP treatment delays ≥7 days (4% of cycles, 13% of patients), doxorubicin, and/or cyclophosphamide dose reductions (1% of cycles, 6% of patients) or (R)CHOP discontinuations due to toxicity (4% of patients) were uncommon. Neutropenic fever (NF) occurred in 7% of cycles and 24% of patients and was more common during HDMTX-containing cycles. Acute kidney injury (AKI) occurred in 19% of cycles but was mostly grade ≤2. Grade ≥3 hepatotoxicity and mucositis were uncommon (each 2% of cycles). In the prophylaxis cohort, the rates of NF and grade ≥2 AKI were lower in patients who initiated HDMTX with cycle 2 or later (11% vs 30%, P = .03 and 16% vs 39%, P = .03, respectively). Our data show that HDMTX administration on day 1 of (R)CHOP may improve the deliverability of (R)CHOP and the overall safety of the regimen compared with historical data of HDMTX administration on day 10 or later of R-CHOP. Delaying prophylactic HDMTX beyond cycle 1 of (R)CHOP may reduce the risk of NF and AKI.
Introduction
Secondary central nervous system (CNS) involvement in non-Hodgkin lymphoma (NHL) is associated with poor outcomes and remains a major therapeutic challenge.1,2 IV high-dose methotrexate (HDMTX) achieves excellent blood-brain barrier penetration and is one of only a few agents that have clinically significant CNS activity in NHL. HDMTX is commonly combined with (R)CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone, with or without rituximab) for the treatment of synchronous CNS and systemic involvement by aggressive NHL. In addition, HDMTX is used to reduce the risk of CNS involvement in patients with diffuse large B-cell lymphoma (DLBCL) identified as having a high risk for CNS relapse based on parameters such as the CNS international prognostic index (CNS-IPI), the number of extranodal sites, involvement of specific high-risk sites, or presence of MYC and BCL2 double-expression by immunohistochemistry (IHC), and in patients with high-grade B-cell lymphoma (HGBCL) harboring MYC with BCL2 and/or BCL6 rearrangements by fluorescence in situ hybridization (FISH).3-5 In the prophylactic setting, HDMTX is commonly administered after R-CHOP treatment completion or concurrently with R-CHOP.3 Because CNS relapses in DLBCL commonly occur shortly after, or even during frontline therapy, with a median time from diagnosis to CNS relapse of 6 to 9 months,1,6-11 there is rationale to administer HDMTX concurrently with R-CHOP early in the course of treatment. However, the additional toxicity from the concurrent administration of HDMTX may compromise the dose intensity of the primary treatment (R-CHOP). This can be a particular concern as R-CHOP dose intensity is an independent predictor of outcomes in DLBCL, whereas the overall risk of CNS relapse is relatively low in comparison.3,12 Whether used for treating known CNS involvement or as prophylaxis, it is imperative that HDMTX be administered in a manner that minimizes toxicity and preserves treatment dose intensity.
In most published studies on the use of HDMTX concurrently with R-CHOP in which the timing of HDMTX administration was reported, HDMTX was administered midcycle, between days 10 and 15 following R-CHOP.6,13-16 This interposition of methotrexate and other antimetabolites between chemotherapy cycles (including CHOP) in NHL dates back to more than 4 decades. To improve the efficacy of standard treatments, the antimetabolites, which are most effective during the S-phase of cell division, were added between chemotherapy cycles when the tumor burden is reduced and cells are in the logarithmic growth phase.17-20 It has since become evident that the main therapeutic role of methotrexate in NHL is treating or preventing CNS involvement rather than improving the treatment of systemic disease. Recently, an international multicenter retrospective study by Wilson et al of 334 patients with DLBCL who received CNS prophylaxis with HDMTX, of whom 204 patients received concurrent HDMTX and R-CHOP, demonstrated differences in toxicity and tolerability related to the timing of HDMTX during the R-CHOP cycle.14 Wilson et al found that HDMTX administration midcycle (on or after day 10 of R-CHOP) is associated with higher rates of R-CHOP treatment delays, presumably due to toxicities, compared with its administration earlier in the R-CHOP cycle (26% vs 16%, P = .01). However, most patients in this study received HDMTX between days 7 and 9 of R-CHOP, with <5% of patients between days 1 and 3. Whether HDMTX administration earlier than day 7 of R-CHOP further reduces toxicity and improves R-CHOP deliverability is unknown. In this study, we report our experience with HDMTX administration on day 1 of (R)CHOP as we have routinely used it for prophylaxis against or treatment of CNS involvement in aggressive NHL.
Methods
Study design and patient population
In this retrospective study, we included consecutive patients with aggressive NHL who received at least 1 cycle of HDMTX (at least 1.5 g/m2) in combination with (R)CHOP at the James Cancer Hospital of The Ohio State University (OSU) from January 2012 through January 2021 under an institutional review board-approved protocol. The study was performed in accordance with the Declaration of Helsinki. We identified patients using pharmacy treatment plan records and the OSU Lymphoma Database; the latter is a prospectively maintained database of patients with lymphoma treated at our institution. Patients who were incarcerated and those with inadequate records were excluded. We grouped patients into 2 cohorts based on the indication for HDMTX use: prophylaxis against CNS involvement (prophylaxis cohort, HDMTX-P) and treatment of known CNS involvement (treatment cohort, HDMTX-T). The decision to use HDMTX for CNS prophylaxis, number of HDMTX cycles administered for prophylaxis against or treatment of CNS involvement, and baseline CNS evaluation (brain and/or spine magnetic resonance imaging [MRI] and cerebrospinal fluid [CSF] analysis) were at the treating physician’s discretion.
Study aims
The primary aim of this study was to evaluate HDMTX tolerability when administered on day 1 of (R)CHOP. First, we assessed (R)CHOP deliverability by evaluating the rates of (R)CHOP therapy delays of ≥7 days due to toxicity (based on standard 21-day cycles), doxorubicin and/or cyclophosphamide dose reductions, and (R)CHOP premature discontinuations. In addition, we calculated doxorubicin and cyclophosphamide relative-dose intensities (RDIs) for patients in the HDMTX-P cohort. Second, we evaluated the rates of selected toxicities, including acute kidney injury (AKI), hepatotoxicity (grade ≥3 elevations in hepatic transaminases or bilirubin), neutropenic fever (NF), and grade ≥3 mucositis. Severity was graded according to the NCI Common Terminology Criteria for Adverse Events (CTCAE), Version 5.0. Disease-related and survival outcomes including objective response rate, complete response rate, progression-free survival (PFS), cumulative incidence of CNS progression/relapse, and overall survival (OS) were evaluated as secondary aims.
Data collection
Patient characteristics, laboratory data, and clinical outcomes were extracted from the OSU Lymphoma Database and manually from the electronic medical record (EMR). Treatment regimen details, including dates of administration and doses of HDMTX and components of (R)CHOP, were collected through the pharmacy treatment plan records and the EMR. Complete blood counts (CBCs), chemistries, and appropriately timed methotrexate levels were obtained at least once daily for inpatients receiving HDMTX with (R)CHOP and typically twice weekly following discharge. Because (R)CHOP cycles completed in the outpatient setting (most cycles without HDMTX) had CBC and chemistries obtained only on the day of treatment of most patients, laboratory-based adverse events (AKI and hepatotoxicity) were evaluated for HDMTX-containing cycles only. NF and mucositis were collected for all cycles via review of clinic notes and emergency department or inpatient encounters. The RDIs of doxorubicin and cyclophosphamide were calculated for patients in the HDMTX-P who received ≥2 consecutive (R)CHOP cycles (with or without HDMTX) to capture the cumulative dose received and incorporate all delays in therapy, including those for reasons other than toxicity. RDI was calculated by dividing the ratio of the actual cumulative dose (in mg/m2) of each agent received over the actual time period over which the regimen was given by the expected dose received (50 mg/m2 per cycle for doxorubicin and 750 mg/m2 per cycle for cyclophosphamide) over the expected time period (based on 21-day cycles).
Statistical analysis
Baseline patient characteristics were summarized by descriptive statistics with median and range presented for continuous variables and frequency count and percentage provided for categorical variables. Treatment and toxicity data were shown per cycle and presented through descriptive statistics. Cycle-level toxicity data were further aggregated into patient-level data to show general toxicity patterns. Fisher’s exact test was used to compare toxicity rates among patients in the HDMTX-P cohort who received their first cycle of HDMTX with their first cycle of (R)CHOP vs those who started HDMTX during later cycles, with P values < .05 considered statistically significant. Univariable logistic regression models were built to estimate the association between patient characteristics and outcomes. PFS was calculated from the time of diagnosis to either progression or death, and OS was calculated from the time of diagnosis to death due to all causes; patients without events were censored at the time of the last follow-up. PFS and OS were estimated through the Kaplan-Meier method. Cumulative incidence of CNS relapse was calculated with non-CNS relapse or death as the competing risk and estimated through cumulative incidence function.
Results
Patients
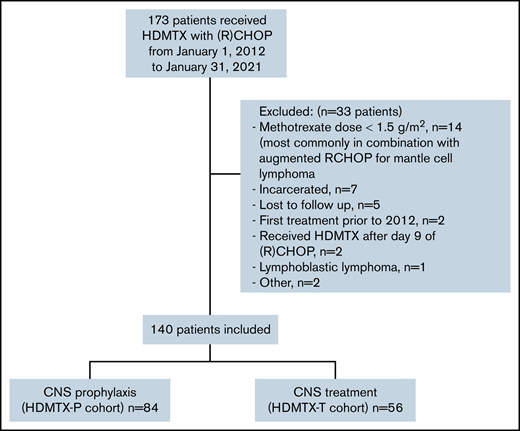
Of 914 patients with lymphoma treated with (R)CHOP at our institution from January 2012 through January 2021, 173 patients received concurrent IV methotrexate, and 140 patients were included in the analysis. Eighty-four patients (60%) received HDMTX for prophylaxis against CNS disease (HDMTX-P cohort) and 56 patients (40%) for treatment of CNS disease (HDMTX-T cohort) (Figure 1). The most common reason for exclusion was patients receiving methotrexate doses <1.5 mg/m2. Baseline characteristics for the HDMTX-P and HDMTX-T cohorts, as well as the overall cohort, are listed in Table 1.
In the HDMTX-P cohort, the median age was 58 years (range 19 to 76), and 68% were male. Most patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1 (91%). Seventy-nine patients had DLBCL (94%) and 5 patients (6%) had HGBCL, including 2 patients (2%) with double-hit lymphoma. MYC and BCL2 double-expression by IHC was present in 50% of patients (available for 64% of patients, n = 54). The IPI score classified 60% and 31% of patients as having intermediate- or high-risk disease, respectively. The median number of extranodal sites was 2 (range 0 to 9), with 37% of patients having ≥3 extranodal sites. The most common extranodal sites were renal/adrenal (n = 25, 30%), paraspinal (n = 16, 19%), paranasal sinus (n = 10, 12%), and testicular (n = 8, 10%). The CNS-IPI score classified 43% and 48% of patients as having intermediate- or high-risk for CNS involvement, respectively. Seven patients with low-risk CNS-IPI received HDMTX for the involvement of high-risk sites (paraspinal n = 3, testicular n = 2, paranasal sinus n = 2). Of the 36 patients with intermediate CNS-IPI, 1 had double-hit lymphoma, 22 had involvement of high-risk sites (paraspinal n = 10, paranasal sinus n = 8, renal/adrenal n = 2, testicular n = 2, breast n = 1), and 6 had involvement of ≥2 extranodal sites with elevated LDH. Laboratory analysis on day 1 of cycle 1 of treatment included albumin serum level ≥3.5 g/dL in 60% of patients, hemoglobin ≥10.0 g/dL in 75%, platelet count ≥150 K/µL in 80%, and absolute neutrophil count (ANC) ≥1500 cells/µL in 94%. Forty-eight patients (57%) had a screening brain MRI before treatment initiation.
In the HDMTX-T cohort, the median age was 62 years (range 19 to 80), and 57% were male. DLBCL was the most common lymphoma subtype (n = 41, 73%) followed by HGBCL (n = 9, 16%; including 6 patients with double- or triple-hit lymphoma). Six patients (11%) had peripheral T-cell lymphoma (n = 3), mantle cell lymphoma (n = 2), or primary CNS lymphoma (n = 1). ECOG performance status was 0 or 1 in 64%, 2 in 24%, and 3 in 12% of the patients. The IPI score classified 38% and 55% of patients as having intermediate- or high-risk disease, respectively. The median number of extranodal sites was 2 (range 1 to 7), with 48% of patients having ≥3 extranodal sites. The most common extranodal sites outside the CNS were renal/adrenal (n = 7, 13%), paraspinal (n = 6, 11%), and testicular (n = 4, 7%). CNS involvement was parenchymal in 15 patients (27%), leptomeningeal in 31 (56%), or both in 9 (16%) (missing for 1 patient). Labs on day 1 of cycle 1 of treatment included albumin serum level ≥3.5 g/dL in 26% of patients, hemoglobin ≥10.0 g/dL in 62%, platelet count ≥150 K/µL in 70%, and ANC ≥1500 cells/µL in 90%.
Treatment
A total of 714 chemotherapy cycles were evaluated: 445 cycles in the HDMTX-P cohort and 269 in the HDMTX-T cohort (Table 2). All chemotherapy cycles were CHOP except for 3% (n = 21) that were dose-adjusted EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin), none of which were combined with HDMTX. Rituximab was given in all but 3 patients (2 had T-cell lymphoma and 1 had hepatitis B infection). Approximately half (54%, n = 242) of the cycles in the HDMTX-P cohort and 90% (n = 241) in the HDMTX-T cohort included HDMTX, for a total of 483 HDMTX-containing cycles. HDMTX starting dose was 3.5 g/m2 in all but 4 patients (range 1.5 to 3 g/m2). HDMTX was administered on day 1 of (R)CHOP in all HDMTX-containing cycles but 4 (3 cycles on day 2 and 1 on day 8). The median numbers of HDMTX-containing cycles administered per patient in the HDMTX-P and HDMTX-T cohorts were 3 (range 1 to 6) and 5 (range 1 to 6), respectively. Five patients in the HDMTX-P cohort received 5 or 6 HDMTX-containing cycles: 2 patients with nasopharyngeal and/or retro-orbital (but not intraocular) involvement, 1 with primary testicular, 1 with spinal cord compression, and 1 for suspected sixth cranial nerve palsy with negative brain MRI and CSF analysis. HDMTX was administered with the first cycle of treatment in 55% of patients in the HDMTX-P cohort, 70% in the HDMTX-T cohort, and 61% overall. Intrathecal (IT) methotrexate was administered in 8% of the cycles in the HDMTX-P cohort (n = 35) and 12% in the HDMTX-T cohort (n = 31). Granulocyte colony-stimulating factor (G-CSF) was given in 90% of cycles overall (86% and 95% in the HDMTX-P and HDMTX-T cohorts, respectively) and 99% of HDMTX-containing cycles. Treatment with (R)CHOP was followed by consolidative stem cell transplantation (SCT) in 5 patients (6%) in the HDMTX-P cohort (all autologous) and 17 patients (30%) in the HDMTX-T cohort (15 autologous and 2 allogeneic, including 14 autologous and 1 allogeneic in patients with DLBCL/HGBCL).
(R)CHOP deliverability
Cycle-level and patient-level toxicity data are shown in Tables 3 and 4. Overall, only 23 cycles (4%) were delayed by ≥7 days due to toxicity, with a median delay of 8 days (range 7 to 33); 11 cycles (3%) in the HDMTX-P cohort (median 7 days, range 7 to 14), and 12 cycles (6%) in the HDMTX-T cohort (median 8, range 7 to 33). Most delayed cycles (n = 19, 83%) were preceded by an HDMTX-containing cycle. Eighteen patients (13%) had at least 1 cycle delayed ≥7 days (12% and 14% in the HDMTX-P and HDMTX-T cohorts, respectively). The most common reasons for delays overall were infection/NF (43%) and myelosuppression (26%). Dose reductions in doxorubicin and/or cyclophosphamide relative to the previous cycle occurred in 9 cycles (1%), with 4 of these preceded by an HDMTX-containing cycle. The median RDI of each of doxorubicin and cyclophosphamide in the HDMTX-P cohort was 1.00 (range 0.45 to 1.00 for doxorubicin and 0.47 to 1.00 for cyclophosphamide). The RDI of each of doxorubicin and cyclophosphamide in the HDMTX-P cohort was ≥0.70 in 98% of patients and ≥0.90 in 90% of patients. (R)CHOP was prematurely discontinued in 23 patients (16%); 7 patients (8%) in the HDMTX-P cohort and 16 patients (29%) in the HDMTX-T cohort, most commonly due to toxicity in the HDMTX-P cohort (n = 4, 57%) and disease progression/death in the HDMTX-T cohort (n = 14, 88%). Overall, 5 patients (4%) discontinued (R)CHOP treatment prematurely due to toxicity. HDMTX was prematurely discontinued due to toxicity, without or before (R)CHOP discontinuation, in 15 patients (11%); 11 (13%) and 4 (7%) patients in the HDMTX-P and HDMTX-T cohorts, respectively.
Toxicities
NF occurred in 33 patients (24%) and 51 cycles (7%) overall; 18 patients (21%) and 27 cycles (6%) in the HDMTX-P cohort and 15 patients (27%) and 24 cycles (9%) in the HDMTX-T cohort. An HDMTX-containing cycle preceded 70% and 100% of NF events in the HDMTX-P and HDMTX-T cohorts, respectively. Twenty-three (45%) of the 51 NF events occurred during the first treatment cycle (48% and 41% in the HDMTX-P and HDMTX-T cohorts, respectively). All patients in the HDMTX-T cohort and 11 (85%) of the 13 patients in the HDMTX-P cohort who developed NF during the first treatment cycle received HDMTX on that cycle. Further, in the HDMTX-P cohort, patients were more likely to develop NF during their whole treatment course if HDMTX was initiated with the first treatment cycle (30%, 14 of 46 patients) compared with those who initiated HDMTX in cycle 2 or later (11%, 4 of 38 patients) (P = .03). In a logistic regression analysis done to examine variables associated with the risk of NF over the treatment course in the HDMTX-P cohort, administration of HDMTX with the first treatment cycle was associated with a higher risk (odds ratio [OR] 3.72, 95% confidence interval [CI] 1.11-12.49, P = .03) (Table 5) . Hemoglobin level was the only other variable associated with NF with higher levels on day 1 of the first treatment cycle and day 1 of the first HDMTX-containing cycle being associated with a lower risk (OR 0.65, 95% CI 0.48-0.88, P = .005 and OR 0.70, 95% CI 0.51-0.95, P = .02, respectively).
AKI occurred in 61 patients (44%) and 92 cycles (19% of HDMTX-containing cycles) overall; 32 patients (38%) and 42 cycles (17%) in the HDMTX-P cohort and 29 patients (52%) and 50 cycles (21%) in the HDMTX-T cohort. Overall, the majority of AKI events were grade 1 (5%) or 2 (11%), with grades 3 and 4 occurring in 2% and <1% of cycles, respectively (1% and 0% in the HDMTX-P cohort and 3% and 1% in the HDMTX-T cohort). Glucarpidase was used in 8 cycles (2%), 3 in the HDMTX-P cohort and 5 in the HDMTX-T cohort. Similar to NF, grade ≥2 AKI was more common in patients who initiated HDMTX with the first treatment cycle (39%, 18 of 46 patients) compared with those who initiated HDMTX in cycle 2 or later (16%, 6 of 38 patients, P = .03). Grade ≥3 elevations in hepatic transaminases occurred with 11 HDMTX-containing cycles (2%); 5 (2%) and 6 (2%) cycles in the HDMTX-P and HDMTX-T cohorts, respectively. Grade ≥3 mucositis occurred in 17 cycles (2%); 7 (2%) and 10 (4%) in the HDMTX-P and HDMTX-T cohorts, respectively. The rate and severity of toxicities in the 5 patients in the HDMTX-P cohort who received 5 or 6 cycles of HDMTX were similar to the rest of the cohort (data not shown).
Disease-related outcomes
In the HDMTX-P cohort, the objective response rate following HDMTX and (R)CHOP was 91%, including complete response in 90%. With a median follow-up of 23 months (range 3 to 90), the 2-year PFS and OS rates were 72% (95% CI 60%-81%) and 93% (95% CI 81%-97%), respectively (Figure 2) . Six patients had CNS progression with a 2-year cumulative incidence of CNS progression of 9% (95% CI 4%-18%). Of these 6 patients, 5 had leptomeningeal involvement, 1 had both parenchymal and leptomeningeal involvement, and 3 had concurrent systemic relapse/progression. Baseline characteristics for these 6 patients include intermediate-risk CNS-IPI in 3 patients, high-risk CNS-IPI in 3 patients, double-hit status in 1 patient, MYC and BCL2 double expression by IHC in 3 patients (available for 5), and high-risk site involvement in 2 patients (breast and paranasal sinus). Four of these patients had screening brain MRI and diagnostic lumbar puncture (with cytology and flow cytometry) done at diagnosis, and 1 patient received IT methotrexate. All of the 5 patients in the HDMTX-P cohort who received 5 or 6 cycles of HDMTX achieved complete response and none of them relapsed. The predicted 2-year rate of CNS involvement in the prophylaxis cohort based on the CNS-IPI risk score is 6.4%.
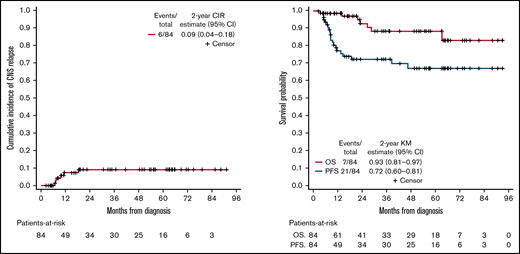
Cumulative incidence of relapse, PFS, and OS in patients with DLBCL and HGBCL receiving prophylactic HDMTX.
Cumulative incidence of relapse, PFS, and OS in patients with DLBCL and HGBCL receiving prophylactic HDMTX.
For patients with DLBCL or HGBCL in the HDMTX-T cohort (n = 50), the objective response rate following HDMTX and R-CHOP was 66%, including complete response in 60%. With a median follow-up of 28 months (range 2 to 100), the 2-year PFS and OS rates were 43% (95% CI 28%-57%) and 57% (95% CI 41%-70%), respectively (Figure 3). Twelve patients had CNS relapse/progression with a 2-year cumulative incidence of CNS progression/relapse of 26% (95% CI 14%-40%). CNS relapse/progression was parenchymal in 6 patients, leptomeningeal in 4, and both in 2. Of patients with CNS relapse/progression, 1 had concurrent CNS and systemic progression/relapse, and 11 had CNS progression/relapse only. Eight patients relapsed/progressed systemically without CNS involvement.

Cumulative incidence of CNS relapse/progression, PFS, and OS in patients with DLBCL and HGBCL with known CNS involvement.
Cumulative incidence of CNS relapse/progression, PFS, and OS in patients with DLBCL and HGBCL with known CNS involvement.
Discussion
To our knowledge, this is the largest study to report on the safety and deliverability of HDMTX administered on day 1 of (R)CHOP. Other studies on HDMTX administration on day 1 of R-CHOP include a small study of 7 patients with primary CNS lymphoma and another study of 57 patients with aggressive B-cell NHL (the latter did not include safety data).21,22 Our data of 140 patients with aggressive NHL treated with HDMTX on day 1 of (R)CHOP show that the majority of patients were able to receive treatment as planned. (R)CHOP treatment delays ≥7 days (4% of cycles, 13% of patients), doxorubicin and/or cyclophosphamide dose reductions (1% of cycles, 6% of patients), or (R)CHOP treatment discontinuations due to toxicity (4% of patients) were uncommon. Further, the RDIs of each of doxorubicin and cyclophosphamide in the HDMTX-P cohort were more than 0.90 in 90% of patients. In terms of toxicities, NF occurred in 7% of cycles and 24% of patients, which is a slightly higher rate than what is reported in retrospective and prospective studies of patients with DLBCL treated with R-CHOP alone (11% to 19% of patients) despite the more liberal use of G-CSF in our study (90% of cycles overall, 99% of HDMTX-containing cycles).13,23-28 The fact that the majority (84%) of NF events in our study were preceded by an HDMTX-containing cycle (68% of cycles overall contained HDMTX) suggests that concurrent HDMTX administration with (R)CHOP increases the risk of NF. The rate of AKI was relatively high in our study (19% of cycles), but the majority of cases were grade ≤2. Lastly, the rates of grade ≥3 hepatotoxicity and mucositis were low (each 2% of cycles). Importantly, although patients in our study had very high-risk disease features, they represent a group of selected patients deemed fit to receive HDMTX with a median age of 60 years and adequate baseline hematologic and renal function, and the majority (76%) had ECOG PS of 0 to 1.
The toxicity results of our HDMTX-P cohort compare favorably overall with those of patients treated with concurrent HDMTX and R-CHOP in the study by Wilson et al (n = 204 patients, 409 concurrent HDMTX and R-CHOP cycles, all for CNS prophylaxis). However, there are important differences in the patient characteristics and study methodology between the 2 studies. A higher proportion of patients in the study by Wilson et al had ECOG PS of ≥2 (22% vs 8%), but they received fewer HDMTX-containing cycles per patient (median of 2, range 1 to 4) compared with our study (median of 3, range 1 to 6). Wilson et al reported treatment delays of any duration but only for R-CHOP cycles that followed HDMTX, and collected toxicity data (NF, AKI, grade ≥2 hepatotoxicity, any grade mucositis) only in HDMTX-containing cycles. In contrast, we reported treatment delays and collected data on NF and mucositis throughout all cycles regardless of HDMTX administration. However, we only included treatment delays ≥7 days, as we believe these are more clinically relevant. With these limitations in mind, in the study by Wilson et al, 20% of R-CHOP cycles following HDMTX were delayed (median 7 days, range 2 to 150), which was more common when HDMTX was administered on day ≥10 of R-CHOP (26% vs 16%, P = .01). This compares with 3% of cycles delayed ≥7 days in our HDMTX-P cohort (median 7 days, range 7 to 14). At the patient-level data, 32% of patients in the study by Wilson et al had at least 1 R-CHOP cycle delayed for ≥7 days compared with 12% in our HDMTX-P cohort. Notably, the rate of AKI was higher in our study (17% vs 5%), driven mainly by a higher rate of grade 2 AKI (10% vs 1%). It is plausible that the risk of AKI when HDMTX is administered on day 1 of (R)CHOP is higher, especially during the first treatment cycle when other risk factors for AKI (for example, tumor lysis syndrome) or factors associated with higher risk for HDMTX-related nephrotoxicity (for example hypoalbuminemia) are more likely to be present.29,30 Not only did patients in our HDMTX-P cohort receive more HDMTX cycles during the first treatment cycle (55% vs <40%), they also received more HDMTX-containing cycles per patient overall. The definition of AKI was also different between the studies; we defined grade 2 AKI as creatinine increase >1.5 to 3.0 times the upper limit of normal per CTCAE V5.0, whereas Wilson et al defined it as creatinine 2 to 2.9 times baseline per KDIGO criteria. The rate of NF was slightly lower in our study (6% vs 10% of cycles). The rate of hepatotoxicity as indicated by AST/ALT elevations was low in both studies (grade ≥3 of 2% in our study vs grade ≥2 of 2% in the study by Wilson et al). We reported grade ≥3 mucositis in 2% of cycles compared with any grade mucositis in 10% of cycles in the study by Wilson et al. Finally, the 2-year cumulative incidence of CNS progression of 9% seen in our study is in line with results from recent studies of prophylactic HDMTX in patients with DLBCL, including the study by Wilson et al (2 to 5 year cumulative incidence of 7% to 12%).11,13,22,31,32 Overall, our study confirms and extends the findings by Wilson et al that scheduling concurrent HDMTX early in the course of the R-CHOP cycle may be better tolerated. Our retrospective analysis does not provide a biological explanation for this observation. We hypothesize that earlier HDMTX administration may provide the bone marrow (BM) more recovery time before the next (R)CHOP cycle, thereby reducing the need to delay the subsequent cycle due to prolonged myelosuppression or related toxicities.
Our data show that initiating prophylactic HDMTX after the first cycle of R-CHOP may be safer. Consistent with other studies, the rate of NF in our study was highest during the first (R)CHOP cycle.24,27,28,33,34 However, the vast majority of NF events that occurred during the first treatment cycle in both cohorts were in patients who received HDMTX during that cycle, which was disproportionate to the percentage of patients who received HDMTX in the first cycle. Further, in the HDMTX-P cohort, the rate of NF throughout the whole treatment course was lower in patients who initiated HDMTX on cycle 2 or later (11% vs 30%, P = .03). Regression analysis of different patient- and treatment-related factors in the HDMTX-P cohort identified initiation of HDMTX on the first treatment cycle and lower hemoglobin level as the only factors being associated with increased risk of NF. Similarly, the rate of grade ≥2 AKI was lower in patients in the HDMTX-P who initiated HDMTX on cycle 2 or later (16% vs 39%, P = .03). These findings may be attributed to the higher disease burden seen in patients with aggressive NHL before treatment initiation and support delaying prophylactic HDMTX beyond cycle 1 of R-CHOP to minimize toxicities and preserve treatment dose intensity. This may not apply to patients with known CNS involvement for whom urgent treatment with HDMTX is typically required.
Secondary CNS lymphoma with synchronous CNS and systemic involvement at diagnosis is generally uncommon in aggressive NHL, reported in 5% of patients with DLBCL.35 The optimal treatment in this setting is not well defined, but treatments that target both the systemic and CNS components are required, and outcomes are largely dictated by the ability to treat the CNS disease.36 Limited data in secondary CNS lymphoma and data extrapolated from primary CNS lymphoma have established the role of HDMTX in this setting, with HDMTX concurrently administered with (R)CHOP being one of the most commonly used regimens. To our knowledge, our series of 56 patients with aggressive NHL treated with this regimen for synchronous CNS and systemic involvement is the largest to report its toxicity in this patient population.37 As expected, given differences in the patient baseline characteristics and higher number of HDMTX-containing cycles administered per patient, treatment delays, doxorubicin and/or cyclophosphamide dose reductions, and treatment discontinuations, as well as toxicities (NF, AKI, mucositis), were more common in the HDMTX-T cohort than in the HDMTX-P cohort. The rate of grade ≥3 AKI was particularly high, affecting 17% of patients in this cohort. However, despite the higher toxicity rates and higher number of HDMTX-containing cycles per patient administered in the HDMTX-T cohort, HDMTX was more commonly discontinued due to toxicity in the HDMTX-P cohort (13% vs 7%), likely reflecting a higher tolerance by physicians for toxicities related to HDMTX given its crucial role in treating patients with known CNS involvement. For the 50 patients with DLBCL or HGBCL with synchronous CNS and systemic involvement at diagnosis, the 2-year PFS of 43% and OS of 57% reported in our study are in line with outcomes reported in similar retrospective studies showing 2- to 3-year PFS and OS of 42% to 45% and 44% to 56%, respectively.36,38-40 Improved outcomes have been reported with the use of more intensive first-line chemotherapy options, with or without consolidative autologous SCT, in nonrandomized clinical trials that included small numbers of patients with DLBCL or HGBCL with synchronous CNS and systemic involvement at diagnosis.10,41
In addition to its single-center retrospective nature, our study has several limitations. Chart review was limited by missing data, and certain toxicities (for example, mucositis) may not have been consistently recorded in the EMR. Our study lacked a comparator group of patients treated with (R)CHOP alone or with HDMTX administered later in the (R)CHOP cycle. Although we indirectly compared our (R)CHOP deliverability and toxicity data with those of prior studies, there are inherent limitations with any cross-study comparison of this nature. The study was not powered to examine the efficacy of prophylactic HDMTX to reduce the risk of CNS progression. Indications to use prophylactic HDMTX, the number of HDMTX cycles administered in the HDMTX-P and HDMTX-T cohorts, and decisions to delay, dose reduce, or discontinue treatments were not standardized and may reflect variations in individual physician practice.
In conclusion, our data show that HDMTX administration on day 1 of the (R)CHOP cycle is a feasible strategy that results in acceptable (R)CHOP deliverability and compares favorably with separate reports of HDMTX administration midcycle. In addition, incorporation of prophylactic HDMTX starting with R-CHOP cycle 2 or later rather than cycle 1 may reduce the risk of NF and AKI. These findings have important clinical implications for patients with aggressive NHL planned to receive HDMTX in combination with (R)CHOP. Maintaining (R)CHOP dose intensity is a priority as it is associated with better clinical outcomes.12 In addition, better control of systemic disease might reduce the risk of CNS involvement.42,43 In patients with known CNS involvement, maintaining the dose intensity of both HDMTX and (R)CHOP is crucial, as HDMTX is an integral component of the treatment plan. While the use of prophylactic HDMTX to reduce the risk of CNS relapse in DLBCL and HGBCL remains controversial,6,11,13,32,44 our data show a relatively high risk of CNS relapse despite the use of prophylactic HDMTX. However, it is important to note that this was not the primary aim of our analysis. Further studies to validate our findings are required, possibly through multicenter collaborations evaluating different HDMTX administration schedules and strategies.
Acknowledgments
The project described was supported by Award Number Grant UL1TR002733 from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
Authorship
Contribution: M.F., E.D., Y.H., and Y.S. conceived and designed the study, collected and analyzed data, and wrote the manuscript; Y.H. performed statistical analysis; and D.A.B., J.R., N.E., L.A., J.B., B.A.C., R.A.B., and K.M. analyzed/wrote the manuscript.
Conflict-of-interest disclosure: Y.S. has received research funding from BMS, Celgene, TG Therapeutics, and Beigene and has consulted for TG Therapeutics and Epizyme. D.A.B. has consulted for Kite/Gilead. B.A.C. has research funding from Genentech, BMS/Celgene, Triphase, Acerta, Millenium, Merck, Morphosys, and Seattle Genetics and has consulted for Genentech, Verastem, AstraZeneca, and Seattle Genetics. K.M. has received research funding from Pharmacyclis, Novartis, BMS, Celgene, and Merck and has consulted for Pharmacyclics, Janssen, Morphosys, Celgene, Beigene, Epizyme Gilead, Karyopharm, ADC Therapeutics, and Seattle Genetics. All other authors declare no competing financial interests.
Correspondence: Yazeed Sawalha, Department of Internal Medicine, Division of Hematology, The Ohio State University Comprehensive Cancer Center, 1140B Lincoln Tower, 1800 Cannon Dr, Columbus, OH 43210; e-mail: yazeed.sawalha@osumc.edu.