Abstract
Increasing evidence supports the safety and effectiveness of managing low-risk deep vein thrombosis (DVT) or pulmonary embolism (PE) in outpatient settings. We performed a systematic review to assess safety and effectiveness of managing patients with DVT or PE at home compared with the hospital. Medline, Embase, and Cochrane databases were searched up to July 2019 for relevant randomized clinical trials (RCTs), and prospective cohort studies. Two investigators independently screened titles and abstracts of identified citations and extracted data from relevant full-text papers. Risk ratios (RRs) were calculated, and certainty of evidence was assessed using Grading of Recommendations Assessment, Development and Evaluation (GRADE). Seven RCTs (1922 patients) were included in meta-analyses on managing patients with DVT. Pooled estimates indicated decreased risk of PE (RR = 0.64; 95% confidence interval [CI], 0.44-0.93) and recurrent DVT (RR = 0.61; 95% CI, 0.42-0.90) for home management, both with moderate certainty of the evidence. Reductions in mortality and major bleeding were not significant, both with low certainty of the evidence. Two RCTs (445 patients) were included in meta-analyses on home management of low-risk patients with PE. Pooled estimates indicated no significant difference in all-cause mortality, recurrent PE, and major bleeding, all with low certainty of the evidence. Results of pooled estimates from 3 prospective cohort studies (234 patients) on home management of PE showed similar results. Our findings indicate that low-risk DVT patients had similar or lower risk of patient-important outcomes with home treatment compared with hospital treatment. In patients with low-risk PE, there was important uncertainty about a difference between home and hospital treatment.
Introduction
Venous thromboembolism (VTE) includes deep vein thrombosis (DVT) and pulmonary embolism (PE). It is the third most common cardiovascular disorder and affects 2% to 5% of the population during their lifetimes.1,2 The goal of therapy for VTE is to prevent the extension of thrombus and relieve symptoms in the short-term while preventing recurrent events in the long-term. Heparin has been the anticoagulant of choice for treatment of acute VTE.3 More recently, direct oral anticoagulants (DOACs) such as apixaban and rivaroxaban have eliminated the need for low-weight-molecular heparin (LMWH) in acute VTE treatment.
VTE has been traditionally managed in the hospital. However, evidence from several randomized controlled trials (RCTs) as early as the 1990s have indicated that outpatient management may be safe and effective.4,5 These results prompted updates in clinical practice guidelines6,7 The introduction of DOACs for VTE treatment removes the need for injectable coagulants and close laboratory anticoagulant monitoring, making home management even more possible.8 Despite these recommendations and the increasing evidence that home treatment is safe and efficacious, many patients, even those with low risk of complications, are admitted for hospital management.9,10
In this report, we provide a comprehensive and systematic review of the literature and elect to incorporate prospective observational studies in addition to RCTs to determine whether any evidence to avoid home management of DVT or PE exists, particularly among those with “low-risk PE.”
Unlike previous reports, we systematically review the evidence for home management of DVT and PE in 1 report, using standardized inclusion criteria, pooled analysis methods, and assessment of the evidence methods for DVT and PE. We aim to answer the following 2 questions for the American Society of Hematology (ASH) Clinical Practice Guidelines on Treatment of VTE:
Should home treatment vs hospital treatment be used for patients with uncomplicated DVT?
Should home treatment vs hospital treatment be used for patients with PE and low risk of complications?
Methods
This systematic review was performed as part of the ASH Guidelines on Treatment of VTE, developed in partnership with the McMaster University’s Grading of Recommendations Assessment, Development and Evaluation (GRADE) Centre. Review and meta-analysis methodology followed the Cochrane Handbook11 with reporting according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.12
Search strategy
To develop each search strategy, we identified previously published systematic reviews on outpatient management of DVT and PE using Epistemonikos (www.epistemonikos.org). We identified and updated 2 Cochrane systematic reviews, 1 addressing DVT and the other addressing PE.8,13 The number of studies addressing PE was expected to be small and therefore the ASH VTE treatment panel decided to search for prospective observational studies in addition to RCTs for the management of PE. For each search, Medline (1996 to week 3 of July 2019), Embase (1974 to week 3 of July 2019), and the Cochrane Central Register of Controlled Trials (until week 3 of July 2019) were searched. Predefined search terms included “pulmonary embolism” or “pulmonary thromboembolism” or “deep vein thrombosis” and “home treatment” or “outpatient treatment” or “ambulant treatment” or “early discharge.” The searches were restricted to studies of human subjects but not restricted by language. The Medline search strategies are provided in supplemental Material 1. Additionally, the reference lists of relevant studies and reviews were reviewed, and clinical experts in the field of VTE and anticoagulation treatment were consulted for additional references.
Study selection
Two reviewers independently screened titles, abstracts, and the full text of relevant articles based on prespecified inclusion and exclusion criteria. Disagreements were resolved by consensus and by a third reviewer when needed. RCTs and prospective cohort studies were included if they satisfied the following characteristics: included adults ages 18 years and older diagnosed with verified symptomatic uncomplicated DVT or low-risk PE (low-risk PE was classified by any validated or unvalidated measurement tool that aimed to classify mortality risk rate related to PE such as the Pulmonary Embolism Severity Index [PESI]14 ), evaluated the safety and efficacy of home treatment of DVT or PE, or a short hospital admission for up to 72 hours after diagnosis and continued treatment at home past the 72 hours, and used hospital treatment of DVT or PE as the comparison group. Inclusion was not restricted by type of anticoagulant (eg, DOAC or LMWH).
The following outcomes were prioritized as critical for clinical decision-making by the ASH guideline panel: all-cause mortality, PE or recurrent PE, which was considered present if documented objectively, or in case of death in which PE could not be confidently ruled out as a contributing cause, DVT or recurrent DVT, which was considered present if documented objectively. The objective criteria for DVT were either a venous segment of thrombus on ultrasonography or a new intraluminal filling defect on contrast venography. Major bleeding during the first 3 months after the initial DVT or PE diagnosis was defined using the International Society on Thrombosis and Haemostasis (ISTH) criteria.15
To answer question 1 regarding patients with uncomplicated DVT, we included RCTs only. To answer question 2 on patients with PE and low risk of complications, we included RCTs and prospective cohort studies. This decision to include prospective cohort studies was made by ASH panel members given the small number of RCTs identified.
Data abstraction and analysis
One reviewer extracted data from each eligible study using a pretested data abstraction form, and data were checked by another reviewer to assess accuracy. Disagreements were resolved by discussion, and by a third reviewer when needed. The data collected included patient characteristics including age and sex, intervention and control group details, mean hospital length of stay, and duration of follow up. Risk ratios (RRs) and 95% confidence intervals (CIs) were calculated by pooling the results from RCTs using the Mantel-Haenszel method and the random effects model. Heterogeneity was assessed using the I2 index and was deemed as moderate to high with an I2 over 50%.11 Data were analyzed using RevMan 5.3. Two reviewers evaluated the certainty of the evidence for each outcome using the GRADE approach.16 The certainty of the evidence was assessed as high, moderate, low, or very low and summarized in a GRADE Evidence Profile.16
Risk of bias
Information on risk of bias was collected and assessed for each outcome in each included study using the Cochrane risk of bias tool for RCTs.11 The Cochrane risk of bias tool was adapted for prospective observational studies. The following items were included: adequate assessment of exposure, clear selection for home treatment, adequate study population, adequacy of follow-up and assessment of outcome. Assessment of exposure was considered adequate when the index PE was diagnosed with 1 of the following imaging techniques: pulmonary angiography, computed tomography angiography, high probability ventilation-perfusion (V/Q) scan or intermediate probability V/Q scan combined with a positive compression ultrasonography for DVT. An unambiguous selection for home treatment was present if predefined exclusion criteria were used to select whether a patient could be treated as an outpatient. A study population was considered adequate if it consisted of consecutive patients or included a random sample of all potentially eligible patients. Complete follow-up was required in at least 80% of patients for follow-up to be considered adequate. Assessment of outcome was adequate when objective criteria were used, comparable to the international criteria for assessing recurrent VTE or major bleeding.
Results
Search results
Home vs hospital treatment of uncomplicated DVT.
A total of 452 unique citations were identified from the electronic database search and from other sources. Based on title and abstract screening, 438 citations were excluded. An additional 6 citations were excluded based on full-text screening. A total of 7 studies were included in our systematic review and meta-analysis. Supplemental Material 2 presents the PRISMA diagram.
Home vs hospital treatment of low-risk PE.
A total of 288 and 1435 unique citations were identified from the electronic database searches for RCTs and prospective, observational studies, respectively. Based on title and abstract screening, 271 and 1411 citations were excluded from each search. An additional 15 and 24 citations were excluded based on full-text screening. A total of 2 RCTs and 3 prospective observational studies were included in our systematic review and meta-analysis. Supplemental Material 2 presents the PRISMA diagram.
Study characteristics
Home vs hospital treatment of uncomplicated DVT.
A total of 7 RCTs (1922 patients) investigated hospital vs home treatment of patients with uncomplicated DVT (Table 1).4,5,17-21 Five studies were conducted in France, Greece, Canada, Brazil, and Spain.5,17,18,20,21 The remaining 2 studies were conducted in multiple countries including Australia, New Zealand, Poland, South Africa, The Netherlands, France, and Italy.4,19 One of the 7 studies did not provide details on treatment.21 The remaining 6 reported treating patients in the intervention group with subcutaneous injections of LMWH,4,5,17-20 3 of which stopped LMWH and continued with warfarin at home.5,18,19 One of the 6 studies reported treating patients in the control group with subcutaneous injection of LMWH in the hospital followed by oral anticoagulants,17 the remaining 5 studies reported treating patients with unfractionated heparin (UFH).4,5,18-20 None of the studies reported using DOACs. Length of hospital stay was reported in 4 studies and ranged between 1 and 3 days for the home care group and between 6.5 and 9.6 days for the control group. Duration of follow up ranged from 10 days to 12 months.
Home vs hospital treatment of low-risk PE.
We included 2 RCTs (453 patients)22,23 and 3 prospective observational studies (234 patients)24-26 (Table 2). Studies were conducted in United States, Italy, Spain, and Switzerland.23-26 One study was conducted in multiple countries including Switzerland, France, Belgium, and the United States.22 Assessment of low risk of death to determine eligibility for home treatment varied by study. PESI was used in 1 RCT22 and Hestia criteria were used in the other RCT.23 One of the prospective cohort studies used an unvalidated risk score24 and the remaining 2 studies did not report their methods.25,26 One of the studies included patients treated with DOACs,23 the remaining studies included LMWH and UFH with transition to vitamin K antagonist (VKA) therapy.22,24-26 Little information was reported on defining the intervention (home treatment). In the 2 RCTs home care patients were discharged from the emergency department within 24 hours. The prospective observational studies reported a mean length of hospital stay for home care patients of 3.1 hours in 1 study25 and 0 days in another.26 The third study did not report a hospital length of stay.24 Patients were followed up for 6 months in 1 study and for 3 months in the remaining 4 studies.
Risk of bias
Home vs hospital treatment of uncomplicated DVT.
Among the 7 included RCTs, allocation was clearly concealed in 3 trials.4,5,17 In contrast, concealment was unclear in 3 studies18-20 and probably unconcealed in 1.21 Outcome adjudicators were clearly blinded in the 2 largest RCTs4,5 and unclear in the remaining 5 RCTs.17-21 Missing data were significant in 1 small RCT only.17 A summary of risk of bias for each RCT and associated Forest plots are presented in Figure 1.

Treatment of DVT at home vs in hospital: RCTs. Risk of bias legend: (A) random sequence generation (selection bias);(B) allocation concealment (selection bias); (C) blinding of participants and personnel (performance bias); (D) blinding of outcome assessment (detection bias); (E) incomplete outcome data (attrition bias); (F) selective reporting (reporting bias); and (G) other bias.
Treatment of DVT at home vs in hospital: RCTs. Risk of bias legend: (A) random sequence generation (selection bias);(B) allocation concealment (selection bias); (C) blinding of participants and personnel (performance bias); (D) blinding of outcome assessment (detection bias); (E) incomplete outcome data (attrition bias); (F) selective reporting (reporting bias); and (G) other bias.
Home vs hospital treatment of low-risk PE.
Among the 2 included RCTs, overall risk of bias was low as both studies adequately concealed allocation, blinded outcome adjudicators, and missing data were minimal.22,23 A summary of risk of bias for each RCT and associated forest plots are presented in Figure 2. Among the 3 prospective cohort studies, risk of bias was high due to lack of adjustment for possible confounders, subjective assessment of outcomes, and lack of information on loss to follow-up (supplemental Material 3).24-26
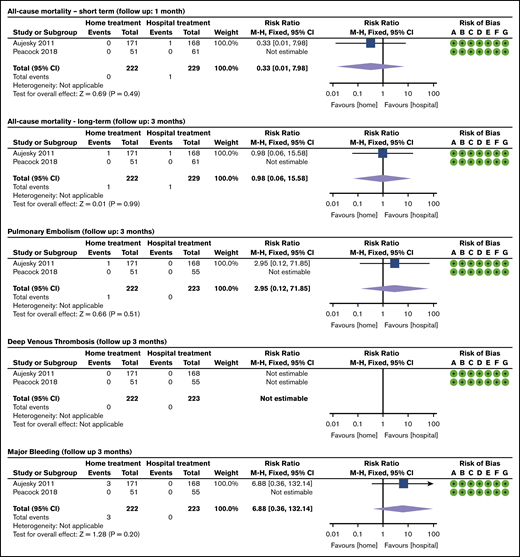
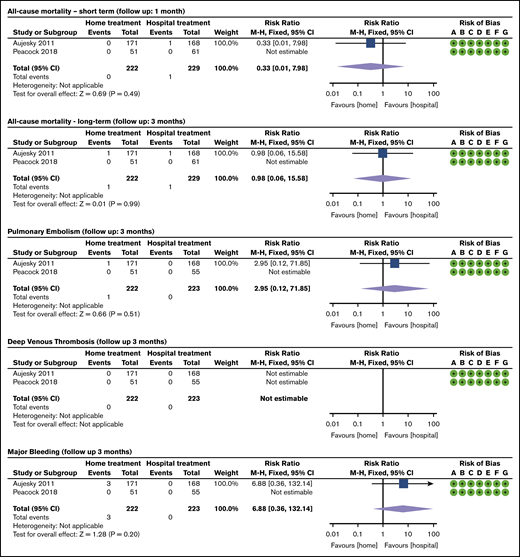
Treatment of PE at home vs in hospital: RCTs. Risk of bias legend: (A) random sequence generation (selection bias); (B) allocation concealment (selection bias); (C) blinding of participants and personnel (performance bias); (D) blinding of outcome assessment (detection bias); (E) incomplete outcome data (attrition bias); (F) selective reporting (reporting bias); and (G) other bias.
Treatment of PE at home vs in hospital: RCTs. Risk of bias legend: (A) random sequence generation (selection bias); (B) allocation concealment (selection bias); (C) blinding of participants and personnel (performance bias); (D) blinding of outcome assessment (detection bias); (E) incomplete outcome data (attrition bias); (F) selective reporting (reporting bias); and (G) other bias.
Synthesis of results
Home vs hospital treatment of uncomplicated DVT
All-cause mortality.
One RCT (214 patients) assessed mortality at 10 days from randomization (short-term mortality). The study reported 0 events in both groups (Figure 1).21 The certainty of the evidence was low because of serious risk of bias and serious imprecision in the anticipated absolute effect (Table 3).21 Six studies (1708 patients) assessed long-term mortality, ranging between 3 months to 12 months from randomization.4,5,17-20 The pooled RR was 0.72 (95% CI, 0.45, 1.15) in favor of home management, and no heterogeneity was observed (I2 = 0; Figure 1).4,5,17-20 The certainty of the evidence, based on the GRADE criteria, was assessed as low because of serious risk of bias, due to lack of allocation concealment and missing data, and serious impression in the anticipated absolute effect (Table 3).4,5,17-21
PE.
Seven RCTs (1922 patients) assessed PE outcomes between 2.1 to 10 days from randomization.4,5,17-21 The pooled RR was 0.64 (95% CI, 0.44, 0.93) in favor of home treatment and no heterogeneity was observed (I2 = 0; Figure 1).4,5,17-21 The certainty of the evidence was moderate because of serious risk of bias in included studies, due to allocation concealment, unclear blinding of outcome adjudicators, and missing data (Table 3).4,5,17-21
Recurrent DVT.
Six studies (1708 patients) assessed recurrent DVT of the upper leg outcomes between 2.1 to 10 days from randomization.4,5,17-20 The pooled RR was 0.61 (95% CI, 0.42, 0.90) in favor of home treatment and no heterogeneity was observed (I2 = 0; Figure 1).4,5,17-20 The certainty of the evidence was moderate because of serious risk of bias in included studies, due to allocation concealment, unclear blinding of outcome adjudicators, and missing data (Table 3).4,5,17-20
Major bleeding.
Seven RCTs (1922 patients) assessed major bleeding between 2.1 to 10 days from randomization.4,5,17-21 The pooled RR was 0.67 (95% CI, 0.33, 1.36) in favor of home management, and no heterogeneity was observed (I2 = 0; Figure 1).4,5,17-21 The certainty of the evidence, based on the GRADE criteria, was assessed as low because of serious risk of bias, due to allocation concealment, unclear blinding of outcome adjudicators, and missing data, and serious impression in the anticipated absolute effect (Table 3).4,5,17-21
Home vs hospital treatment of low-risk PE
All-cause mortality.
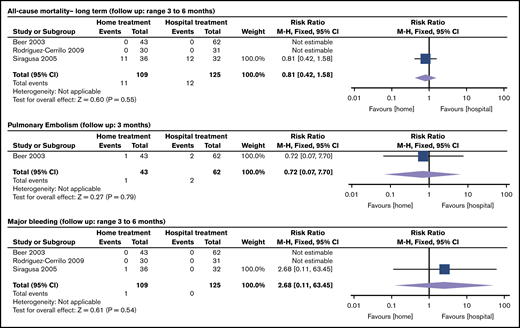
Mortality at 1 month was reported in 2 RCTs (451 patients), 1 of which reported zero events in both groups.22,23 The RR was 0.33 (95% CI, 0.01, 7.87) in favor of home treatment (Figure 2).22,23 The certainty of the evidence was low because of very serious imprecision in the anticipated absolute effect (Table 4).22,23 Mortality at 3 months was reported in 2 RCTs (451 patients) and 3 prospective cohort studies (234 patients).22-26 The pooled RR of home vs hospital care was 0.98 (95% CI, 0.06, 15.58; Figure 2) for RCTs22,23 and 0.81 (95% CI, 0.42, 1.58; Figure 3) for prospective cohort studies.24-26 The certainty of the evidence was low for RCTs because of very serious imprecision in the anticipated absolute effect,22,23 and very low for observational prospective studies because of serious risk of bias, due to the absent reporting of adjustment for potential confounders, assessment of outcomes and adequacy of follow-up for most studies, serious inconsistency, and serious impression in the anticipated absolute effect (Table 4).24-26
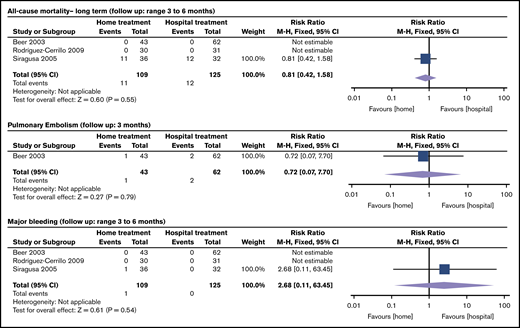
Treatment of PE at home vs in hospital: observational prospective studies. Siragusa et al25 included PE and DVT patients; the meta-analysis presents outcomes for PE patients only.
Treatment of PE at home vs in hospital: observational prospective studies. Siragusa et al25 included PE and DVT patients; the meta-analysis presents outcomes for PE patients only.
Recurrent PE.
Two RCTs (445 patients) assessed recurrent PE at 3 months, 1 of which reported zero events in both groups.22,23 The RR was 2.95 (95% CI, 0.12, 71.85) in favor of hospital treatment (Figure 2).22,23 The certainty of the evidence was low because of very serious imprecision in the anticipated absolute effect (Table 4).22,23 One prospective observational study (105 patients) assessed recurrent PE at 3 months.24 The RR of home vs hospital care was 0.72 (95% CI, 0.07, 7.70) (Figure 3).24 The certainty of the evidence was very low because of serious risk of bias due to the absent reporting of adjustment for potential confounders, assessment of outcomes and adequacy of follow-up for most studies, and serious impression in the anticipated absolute effect (Table 4).24
DVT.
Two RCTs (445 patients) assessed DVT at 3 months.22,23 Both studies reported 0 events in both groups (Figure 2).22,23 The certainty of the evidence was very low because of very serious imprecision in the anticipated absolute effect (Table 4).22,23 DVT was not assessed in any of the prospective observational studies.
Major bleeding.
Two studies (445 patients) assessed major bleeding at 3 months, 1 of which reported zero events in both groups.22,23 The RR was 6.88 (95% CI, 0.36, 132.14) in favor of hospital treatment (Figure 2).22,23 The certainty of the evidence was low because of very serious imprecision in the anticipated absolute effect (Table 4).22,23 Three prospective observational studies (234 patients) assessed major bleeding at 3 months.24-26 The pooled RR was 2.68 (95% CI, 0.11, 63.45) in favor of hospital treatment (Figure 3).24-26 The certainty of the evidence was very low because of serious risk of bias due to the absent reporting of adjustment for potential confounders, assessment of outcomes and adequacy of follow-up for most studies, and very serious impression in the anticipated absolute effect (Table 4).24-26
Discussion
Key findings
Low to moderate certainty evidence suggested that there is no additional risk, and a potential benefit, in managing uncomplicated DVT at home compared with in the hospital. Very low to low certainty evidence suggested there is no clear harm or benefit of managing PE patients with low risk of complications at home. The low quality of evidence among 2 of the 4 outcomes for patients with DVT and among all 4 outcomes for patients with PE was attributed mostly to very serious imprecision in the pooled estimates. Among studies assessing home treatment in DVT patients, results indicated lower risk of PE and recurrent DVT and no lower risk of mortality and major bleeding. The number of studies and sample size of patients assessing home treatment in PE patients were small with few events, and pooled estimates had very wide confidence intervals suggesting no difference in outcomes between home and hospital treatment. Wide confidence intervals were observed in RCTs as well as observational studies.
Implications for clinical practice
This report compiles comprehensive evidence on the efficacy and safety of home management of DVT and PE and includes RCTs as well as observational cohort studies. Our results did not identify any evidence against home management of DVT or PE among patients with low risk of complications. However, observational studies continue to report in hospital management of DVT and PE. An analysis of 652 000 and 394 000 emergency room visits in the US for DVT and PE between 2006 and 2010 indicate that 52% of DVT patients and 90% of PE patients were managed in the hospital.10 Similarly, a more recent analysis of 2387 patients diagnosed with PE across 21 emergency departments between 2013 to 2015 reports that only 7.5% of patients were managed at home.9 Although these observational studies do not stratify by risk of complications, the large number of hospital admission suggests that many patients at low risk of complications are being admitted, despite the evidence favoring outpatient management. Studies in countries outside of the US report higher numbers of outpatient management, however many eligible patients continue to be treated in the hospital. A retrospective analysis of 639 patients with PE and low risk of major hemorrhage indicates that 50% of patients were managed as outpatients.27 This suggests that reasons beyond efficacy and safety may play a role in determining outpatient management of VTE. System level factors maybe influencing decisions for in hospital management of VTE when comparing studies conducted in Canada and the United States. Further, the infrequent use of risk stratification in clinical settings makes implementation of outpatient management for patients with low risk of complications more challenging.
In addition to better or similar efficacy and safety outcomes, home treatment of PE and DVT is cost saving. A matched case control study compared costs accrued over 6 months by patients diagnosed with low-risk VTE and treated at home with rivaroxaban vs usual care with LMWH transitioned to warfarin. Fifty cases and 47 controls were identified. Costs for home treated PE patients were 57% lower than control PE patients (P < .001) and 56% lower for DVT patients (P = .003).28
Our review did not identify any RCTs conducted past 2008 on management of DVT. At the time LMWH during the transition to VKA therapy was the recommended treatment of DVT,6 which requires extensive patient education, access to medications at home, regular subcutaneous injections and routine follow up for laboratory monitoring. Following LMWH, extending treatment with VKA also requires patient’s to be aware of their diet and the administration of other medications due to possible interactions.29 More recent clinical guidelines recommend the use of DOACs which require no subcutaneous injections or routine follow up for laboratory monitoring.7 Theoretically DOAC therapy should make it even easier for patients to be treated at home for DVT resulting in lower costs and less demand for hospital beds. An international multicenter single-arm RCT, published in 2019, investigated early discharge vs hospital treatment of patients with low-risk PE treated with rivaroxaban.16 This study did not fulfill the inclusion criteria in our review, given the single-arm study design. However, results from 525 patients included in planned interim analysis shows that only 3 patients (0.6%) suffered symptomatic non-fatal VTE recurrence. Major bleeding occurred in 6 of the 519 patients (1.2%) comprising the safety population suggesting that early discharge and home treatment with rivaroxaban is effective and safe in carefully selected patients with low-risk PE.30
Strengths and limitations of study
Our report has a few strengths. First, we conducted a comprehensive review of the literature that covers management of DVT as well as PE and that includes evidence from RCTs and observational cohort studies. The review included a systematic search of the literature and independent duplicate screening and data extraction. A second strength is the clinical expertise and methodology input from the ASH VTE treatment panel. Third, we clearly define home management as a short hospital admission for up to 72 hours after diagnosis and continued treatment at home past the 72 hours. Previous studies have not usually clarified this as an inclusion criterion. Previous reviews downgraded the quality of the evidence due to indirectness due to variability in defining home management.8 We excluded studies that reported a longer hospital stay for the intervention arm (home management). Therefore, our final quality of evidence assessment for this outcome was moderate, which will be related to more confidence in the effect estimates.
The small number of included studies, small number of patients in each group, and the very low to moderate certainty of included studies are limitations to this review. This was especially true for evidence regarding PE management, possibly due to low event rates associated with PE. Our search did not identify any new or ongoing RCTs to provide a clear answer for PE management at home. All but 1 of the studies included patients treated with VKA and/or LMWH, only 1 study included patients on DOACs. Due to the small number of studies with patients on DOACs subgroup analysis by type of anticoagulant was not possible. The 1 study that included patients on DOACs23 reported zero events, across all outcomes of interest, in both study groups. This is likely due to the small sample size in the study and the low event rate of these outcomes among patients treated with DOACs. Safety and efficacy are likely greater in DOACs compared with VKA and LMWH13,31 suggesting that including more studies with patients on DOACs will likely show an increased benefit in home treatment of VTE.
Conclusion
Our findings indicate that DVT patients at low risk of complications had similar or lower risk of patient-important outcomes with home treatment compared with hospital treatment. In patients with low-risk PE, there was important uncertainty about a difference between home and hospital treatment.
Send data sharing requests via e-mail to the corresponding author, Yuqing Zhang (zhang363@mcmaster.ca).
Acknowledgments
This systematic review was performed as part of the American Society of Hematology (ASH) guidelines for VTE.
Guideline development was funded by ASH.
Authorship
Contribution: R.K. and Y.Z. contributed to study design, data extraction, statistical analysis, interpretation of results, and writing of the report; S.R., S.A.K., and I.D.F. contributed to study design, search strategy, study selection, data extraction, interpretation of results, and writing of the report; and T.L.O., R.N., I.N., D.M.W., S.S., V.M., R.B., N.P.C., W.W., and H.J.S. contributed to the study design, interpretation of the results, and writing of the report.
Conflict-of-interest disclosure: R.K. received research support from Bristol-Myers Squibb and Takeda. D.M.W received research support and consulting fees from Roche Diagnostics. H.J.S. was the principal investigator for the McMaster GRADE Centre and received funding from ASH that supported this systematic review. The remaining authors declare no competing financial interests.
Correspondence: Yuqing Zhang, Department of Health Research Methods, Evidence and Impact, McMaster University, 1280 Main St W, Hamilton, ON L8S 4L8, Canada; e-mail: madisonz1220@gmail.com or zhang363@mcmaster.ca.