Key Points
Substantially less rpFVIII is administered using an algorithm and given as upfront monotherapy in bleed treatment.
Preexposure porcine inhibitor titer does not predict response and is not a useful marker when dosing using an algorithm-based approach.

Abstract
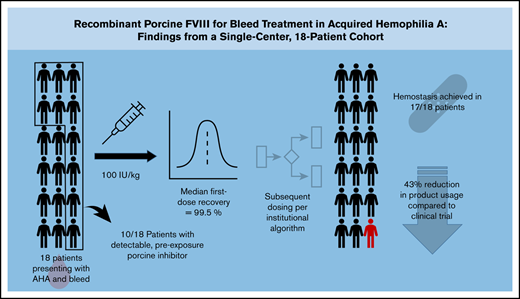
Acquired hemophilia A (AHA) is a rare bleeding disorder in which acquired autoantibodies to endogenous factor VIII (FVIII) decrease FVIII activity and lead to a bleeding phenotype. A substantial majority of individuals who develop AHA present with severe bleeding. Effective treatment requires both immunosuppressive therapy and prompt hemostatic treatment. Bleeding is commonly treated with bypassing agents (BPAs) such as recombinant activated FVII (rFVIIa) or activated prothrombin complex concentrates Disadvantages to BPAs include the inability to monitor response with standard laboratory assays, inconsistent hemostatic efficacy, and thrombosis. Recombinant porcine FVIII (rpFVIII: Obizur, Baxter, Deerfield, IL) was approved by the US Food and Drug Administration (FDA) for bleed treatment in AHA in 2014, and has the advantage of laboratory monitoring of FVIII activity levels and known hemostatic efficacy in the presence of anti-human FVIII inhibitors and after failure of BPAs. Using an algorithm-based approach, rpFVIII has been used to successfully treat 18 patients with AHA at our center with substantially lower doses than the current FDA-recommended dosing. Additionally, data from our cohort show that the preexposure anti-porcine Bethesda titer does not reliably predict the clinical response to rpFVIII treatment and is not correlated with the anti-human Bethesda titer. We also present data showing lower total rpFVIII use for initial bleed resolution when rpVIII is used upfront, as compared with use as rescue therapy. We validated our dosing algorithm, which uses much lower than FDA-recommended doses with 14 more patients than in our previously reported patient series.
Introduction
Acquired hemophilia A (AHA) is an uncommon bleeding disorder in which acquired antibodies to endogenous factor VIII (FVIII) inhibit function of the molecule, leading to decreased FVIII activity and a bleeding phenotype. Effective treatment requires both immunosuppressive therapy (IST) and hemostatic treatment.1-3 The majority of affected individuals present with severe bleeding, most commonly subcutaneous bleeds, muscle bleeds leading to compartment syndrome, and other mucosal bleeding such as epistaxis, gastrointestinal, and genitourinary bleeding.4
Bleed treatment requires prompt attention due to the significant morbidity and mortality associated with bleeding in AHA. Given the extensive experience with bypassing agents (BPAs) such as recombinant activated FVII (rFVIIa) or activated prothrombin complex concentrates (aPCCs), which have similar efficacy and side-effect profiles in retrospective analyses, first-line bleed treatment in AHA is generally with BPAs.5 Disadvantages to BPAs include the inability to monitor response with standard laboratory assays, inconsistent hemostatic efficacy, and thrombosis.3,6-10 Although generally effective, BPAs have a reported failure rate ranging from 7% to 11.6% with rFVIIa, and reported thrombosis rates between 4% and 6.5% with aPCCs and rFVIIa.11-13
A recombinant, B-domain–deleted, porcine FVIII (rpFVIII) was approved by the US Food and Drug Administration (FDA) for treatment of AHA in 2014 (Obizur; Baxter). A phase 2/3 study established the safety and efficacy of dosing rpFVIII for AHA, even in the presence of a preexposure anti-porcine FVIII (pFVIII) inhibitor.1,14,15 This pivotal study used a loading dose of 200 U/kg, basing this on prior data in patients with congenital hemophilia A (cHA) with inhibitors.16 However, rpFVIII displays dynamic pharmacokinetics, and some individuals propose that any treatment of bleeding in AHA start only after determination of human and porcine FVIII inhibitor titers.17-19
We have developed an algorithm-based approach for use of rpFVIII in AHA with a lower starting dose (Figure 1). This approach was used to successfully treat AHA at substantially lower doses than the current FDA-approved dose in a 4-patient series,20 and case reports likewise describe efficacy at lower doses.2,21,22 This algorithm was created based on institution experience and data in patients with cHA and inhibitors, suggesting that doses as low as 50 U/kg could be used in that population in the absence of pFVIII inhibitors.23
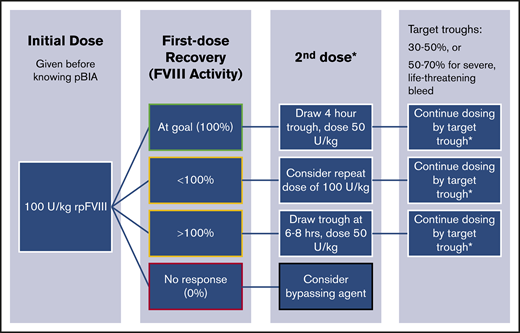
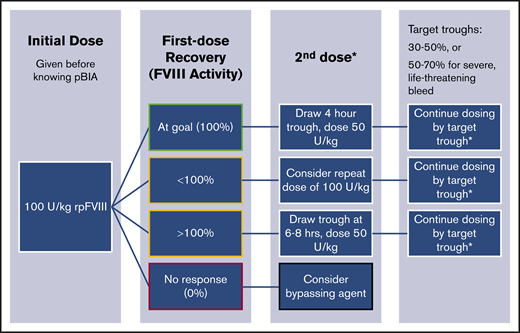
rpFVIII dosing algorithm currently used at our center. At diagnosis or presentation, we obtain a human and porcine BIA (hBIA and pBIA), as well as an FVIII level using a 1-stage clot-based assay (OSCA). Without waiting for the results of the pBIA, we dose rpFVIII at 100 U/kg, and draw a first-dose recovery level (R1) immediately after dosing. If R1 is at target (100% FVIII activity), then a 4-hour trough is obtained. We do not wait for the results of the 4-hour trough, but rather immediately administer a dose for 50 U/kg . If R1 is above target, we then delay drawing a trough until 6 to 8 hours after infusion depending on the degree of FVIII activity. If R1 shows some FVIII activity, but is <100%, we consider a repeat dose of 100 U/kg. Finally, if R1 is 0, we generally recommend changing therapy to a BPAs. Our practice is to dose to a goal trough of 30% to 50% with most bleeds, or 50% to 70% for severe, life-threatening events.
rpFVIII dosing algorithm currently used at our center. At diagnosis or presentation, we obtain a human and porcine BIA (hBIA and pBIA), as well as an FVIII level using a 1-stage clot-based assay (OSCA). Without waiting for the results of the pBIA, we dose rpFVIII at 100 U/kg, and draw a first-dose recovery level (R1) immediately after dosing. If R1 is at target (100% FVIII activity), then a 4-hour trough is obtained. We do not wait for the results of the 4-hour trough, but rather immediately administer a dose for 50 U/kg . If R1 is above target, we then delay drawing a trough until 6 to 8 hours after infusion depending on the degree of FVIII activity. If R1 shows some FVIII activity, but is <100%, we consider a repeat dose of 100 U/kg. Finally, if R1 is 0, we generally recommend changing therapy to a BPAs. Our practice is to dose to a goal trough of 30% to 50% with most bleeds, or 50% to 70% for severe, life-threatening events.
At diagnosis or presentation, we obtain a human and porcine BIA (hBIA and pBIA), as well as a FVIII level using a 1-stage clot-based assay (OSCA). Without waiting for the results of the pBIA, we dose rpFVIII at 100 U/kg, and draw a first-dose recovery level (R1) immediately after dosing. If R1 is at target (100% FVIII activity), then a 4-hour trough is obtained. We do not wait for the results of the 4-hour trough, but rather immediately administer a dose for 50 U/kg. If R1 is above target, we then delay drawing a trough until 6 to 8 hours after infusion depending on the degree of rise in FVIII activity. If R1 shows some FVIII activity, but is <100%, we consider a repeat dose of 100 U/kg. Finally, if R1 is 0, we generally recommend changing therapy to a BPAs. Our practice is to dose to a target trough of 30% to 50% with most bleeds, or 50% to 70% for severe, life-threatening events.
We now report an update to our center’s experience, now having treated 18 patients (17 adults and 1 teen) with AHA with rpFVIII for a total of 24 bleeding episodes, with successful hemostatic outcomes at lower than the FDA-recommended doses, and successful implementation of the above dosing algorithm in the majority of these cases, which allows for rapid dose adjustments and effective therapy even in the presence of detectable porcine inhibitors.
Our algorithmic approach to dosing rpFVIII showed a consistently successful response and is one that utilizes far less than recommended doses and does not require pBIA result to be obtained prior to dosing for effective therapy. We also observed that using rpFVIII as a first-line agent seems to be more effective, with potential cost savings compared with BPAs.
Methods
We extracted, analyzed, and tabulated clinical, pharmacy, and laboratory data from 18 patients treated for a bleed with rpFVIII at the University of North Carolina (UNC) for AHA from July 2015 to February 2019. All patients diagnosed with AHA during this time period were treated according to the dosing algorithm described in the Introduction (Figure 1), with some dose variations per clinician judgement. These patients represent ALL patients with AHA requiring bleed treatment presenting to our institution during this time frame. Investigational review board approval was obtained for our data collection and analysis from the UNC Chapel Hill Institutional Review Board.
All patients were treated with BPAs and/or rpFVIII, and outcomes were all observed by hematology faculty staffing a nonmalignant hematology consult service. All patients were treated with IST, which in our practice includes rituximab and sometimes corticosteroids for acute therapy, although we add cyclophosphamide or mycophenolate mofetil for some patients (Table 1).
We categorized bleeding severity per International Society on Thrombosis and Haemostasis (ISTH) bleeding criteria for clinically relevant nonmajor bleeding (CRNMB) and major bleeding.24 Resolution of bleeding was determined by assessment of clinical, laboratory, and/or radiographic data as appropriate for bleed location and clinical setting.
Results
Of the 18 patients in our cohort, 17 were successfully treated for a bleed. One man was treated with a single dose of rpFVIII unsuccessfully before transitioning to hospice care. In analyzing patient characteristics and response to therapy, we considered the initial encounter at our institution when describing baseline, preexposure laboratory values, including antibody titers. Ten patients were treated for a bleed proximate to their diagnosis, whereas the other 8 were treated for a bleed in the setting of a relapse of known AHA, including cases previously treated for bleeds at another institution, with an intervening “remission” period.
All patients were treated with immunosuppression, with our general practice being to administer rituximab 375 mg/m2 weekly for 4 weeks, with or without corticosteroids, starting at diagnosis; details of immunosuppression are included in Table 1. Seventeen of 18 patients treated for a bleed achieved excellent resolution of their presenting bleed (Table 1). At the time of data analysis, 9 of 18 patients showed complete inhibitor resolution after IST.
Patient demographics are summarized in Table 2. We treated 8 female and 10 male patients. Mean age at time of bleed was 66.6 years (range, 15-85 years). All but 4 of our patients met criteria for severe bleeding (83%), consistent with existing demographic data regarding the presentation and diagnosis of AHA.4 Of those with severe bleeding and for whom a baseline hemoglobin (Hb) was available (9 of 18), a mean decrease in hemoglobin (Hb) of 3.4 g/dL was observed. Eight of the patients had more than 1 bleeding source at diagnosis. The initially treated bleed in our cohort was subcutaneous in 10 patients, muscular in 6 patients (all associated with compartment syndrome), hemarthrosis in 3 patients, GI bleed was present in 4 patients, and 2 presented with hematuria. This distribution is similar to other published data for AHA.4,14 Two patients presented with postoperative bleeding that led to their diagnosis. Four of the 18 patients treated had an identified autoimmune disorder (Table 2).
Laboratory profiles of our cohort are summarized in Table 1. Of our 18 patients, 15 had a pBIA drawn prior to receiving rpFVIII, with 10 of those 15 having a detectable porcine inhibitor at diagnosis. In all patients who had a pBIA drawn, treatment was given prior to knowing the laboratory result. Eight patients were treated with rpFVIII after having first been treated with substantial doses of BPAs. For purposes of analysis, we define “first-line” therapy with rpFVIII even if the patient received rpFVIII within 24 hours of diagnosis, but they could only have received 1 dose of BPAs. We chose this single-dose threshold because many of these patients are transferred to our institution after receiving initial, stabilizing therapy in an outside hospital (usually an emergency department). In the “second-line” therapy group, number of BPA doses ranged from 2 (in a patient on chronic aPCC bleed prophylaxis) to 88 doses of rFVIIa given in a 4-day period (Table 1). In the first-line therapy group, all but 2 patients received rpFVIII as monotherapy, with 1 having had 1 dose of rFVIIa and 1 patient receiving FFP and cryoprecipitate prior to initiating rpFVIII.
Only 2 of the patients in our cohort showed no laboratory response to initial rpFVIII infusion. One of these individuals had also failed multiple BPA infusions and died after trial of a single dose of rpFVIII (no immunosuppression, blood product transfusion, or further factor replacement therapy was attempted). The other patient (patient 9) initially received rVIIa every 2 hours over 4 days unsuccessfully prior to transfer to our institution. At UNC, our standard initial dose of 100 IU/kg rpFVIII was given, with a recovery of 0%. aPCCs was subsequently given without hemostasis for 2 days. IVIg and corticosteroids had also been administered during these 2 days, and a subsequent dose of 200 IU/kg rpFVIII led to therapeutic FVIII activity levels. The initial hBIA in these patients was 17571 and 2533 BU, respectively, the 2 highest hBIA titers observed in our cohort. pBIA in those 2 individuals were 186 and 2.0 BU, respectively. Two patients had suboptimal, yet detectable, laboratory response (peak FVIII activity <50%), but were easily managed with repeat doses per our algorithm (patients 15 and 17; Table 1). The ability to adjust dosing in real time has proven a useful asset in managing these often-difficult cases.
Only 1 patient lost his FVIII response during treatment of the initial bleed and needed subsequent BPA use in the setting of developing a new porcine inhibitor during treatment. Notably, 4 other patients who developed high titer pBIA did not lose their response (1,2, 15,18). Three patients with no preexposure pBIA developed an inhibitor (2, 14, and 15), but only the 1 patient of those 3 lost response to therapy (patient 15). This is in contrast to the clinical trial, in which those who developed an inhibitor on therapy invariably lost their response.14
As shown in Tables 1 and 2, the degree of postexposure pBIA increase is much higher in the individuals who lost response to rpFVIII treatment. There were 9 patients who either had no rise in postexposure pBIA, or whose postexposure pBIA was low-titer (patients 4-7, 9, 12, 16-18). Those in this group with a subsequent bleed all maintained response to rpFVIII. However, of the 7 patients who had a large increase in postexposure pBIA (patients 1-3, 8, 10, 13, and 15), 5 lost response (patients 3, 8, 10, 13, and 15). The 2 exceptions (patients 1 and 2) were clear outliers, despite similar IST. Patient 1 had completed 4 doses of rituximab 15 days prior to a subsequent bleed. Patient 2 had been on 32 days of cyclophosphamide at the time of his subsequent bleed. In contrast, patient 3, who lost response, had only received 2 of 4 planned doses of rituximab at time of subsequent bleed treatment. However, both patients 13 and 15 had received multiple IST medications prior to subsequent bleeds, but had inhibitors resistant to eradication. Patient 10 had completed a course of rituximab 8 days prior to a subsequent bleed during which he lost response to rpFVIII.
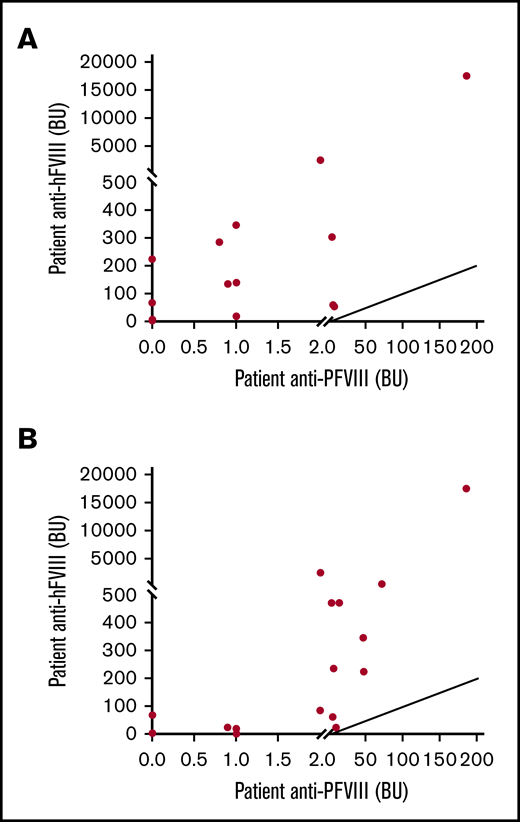
Preexposure pBIA and hBIA were poorly correlated (Spearman coefficient r = 0.5, P = .14; Figure 2A). When comparing postexposure hBIA and pBIA, identified from similarly timed blood draws, correlation is more apparent (Spearman coefficient r = 0.71, P = .002; Figure 2B), perhaps better identified given that only 2 patients never developed pBIA, as opposed to having 5 patients initially with no detectable pBIA (Table 1). Only 5 patients eventually lost their response to rpFVIII during subsequent bleed episodes, 2 of whom had a known autoimmune disorder.
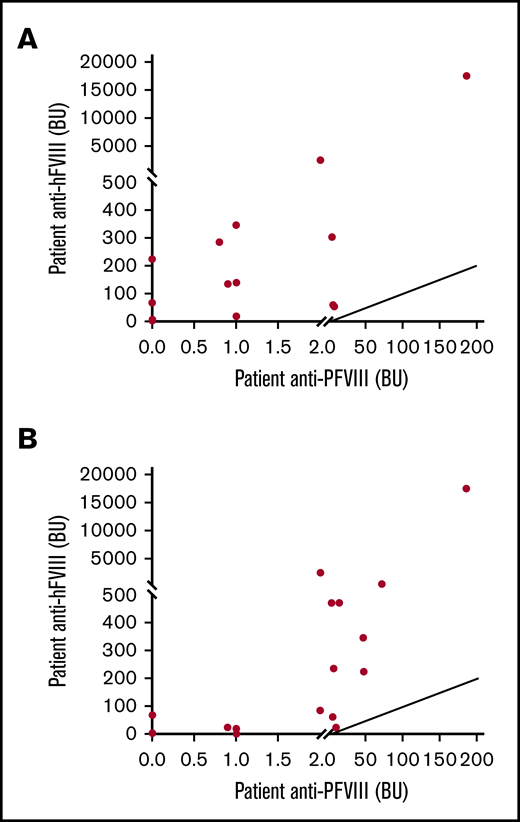
Relationship between anti-hFVIII and anti-pFVIII inhibitors. (A) Correlation between initial anti-hFVIII and anti-pFVIII inhibitors. (B) Correlation between peak anti-hFVIII and anti-pFVIII titer. Initial titers did not correlate (A; Spearman coefficient: r = 0.4; P = .14), although peak human and porcine inhibitor titers had an observable correlation (Spearman coefficient: r = 0.71; P = .002).
Relationship between anti-hFVIII and anti-pFVIII inhibitors. (A) Correlation between initial anti-hFVIII and anti-pFVIII inhibitors. (B) Correlation between peak anti-hFVIII and anti-pFVIII titer. Initial titers did not correlate (A; Spearman coefficient: r = 0.4; P = .14), although peak human and porcine inhibitor titers had an observable correlation (Spearman coefficient: r = 0.71; P = .002).
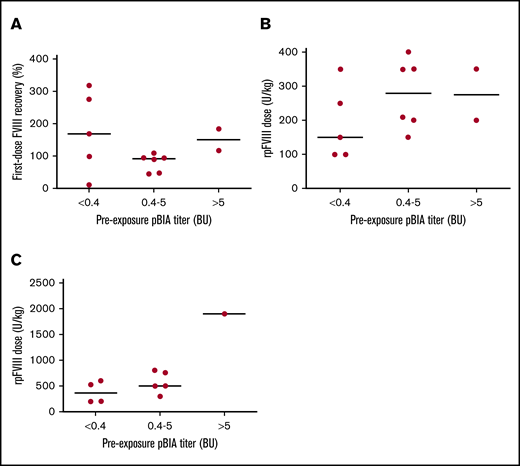
We found no correlation between the preexposure pBIA and FVIII response to initial rpFVIII infusion (Figure 3). This observation held true for the observed first-dose recovery after infusion and total dose given in the first 24 hours; cumulative rpFVIII dose given for the presenting bleed did seem to increase with preexposure pBIA (Figure 3C), though groups are too small to statistically compare. As has been reported, pharmacokinetics were unpredictable, making the algorithm particularly well suited for dosing. For example, based on the algorithm, we were able to rapidly adjust dose and dose interval, with all but 4 patients having FVIII activity greater than 60% in within the first 24 hours (Table 1).
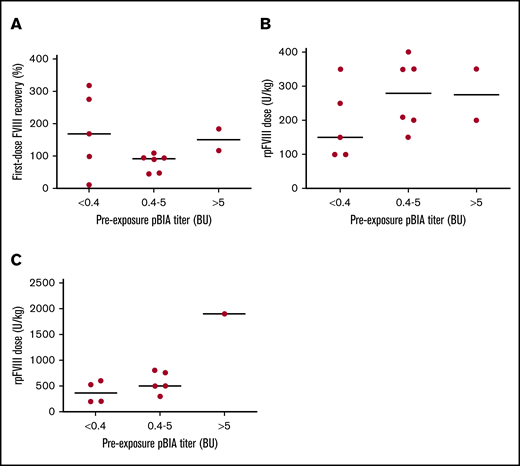
Response to therapy was not predicted by the initial, preexposure, or anti-pFVIII titer. This was observed for several parameters reflecting treatment response, including first-dose recovery FVIII activity after dosing (A), total rpFVIII dose required in the first 24 hours for hemostasis (B), and cumulative rpFVIII dose required for bleed episode (C). There does seem to be a trend up in cumulative rpFVIII dose and the peak anti-pFVIII antibody titer. Note: Three patients did not have a preexposure pBIA and are not included in this figure (Table 1). Patients 7 and 9 received different initial doses than outlined in our algorithm and are likewise not included in these figures. low indicates ≤5 BU; high, >5 BU. (A) First-dose recovery vs preexposure pBIA. (B) rpFVIII dose in first 24 hours vs preexposure pBIA. (C) Cumulative rpFVIII dose for bleed vs preexposure pBIA.
Response to therapy was not predicted by the initial, preexposure, or anti-pFVIII titer. This was observed for several parameters reflecting treatment response, including first-dose recovery FVIII activity after dosing (A), total rpFVIII dose required in the first 24 hours for hemostasis (B), and cumulative rpFVIII dose required for bleed episode (C). There does seem to be a trend up in cumulative rpFVIII dose and the peak anti-pFVIII antibody titer. Note: Three patients did not have a preexposure pBIA and are not included in this figure (Table 1). Patients 7 and 9 received different initial doses than outlined in our algorithm and are likewise not included in these figures. low indicates ≤5 BU; high, >5 BU. (A) First-dose recovery vs preexposure pBIA. (B) rpFVIII dose in first 24 hours vs preexposure pBIA. (C) Cumulative rpFVIII dose for bleed vs preexposure pBIA.
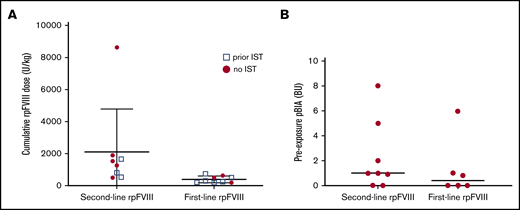
One of the most notable observations in our cohort is in regard to outcome differences in the groups receiving rpFVIII as first-line vs second-line therapy. rpFVIII was given as first-line therapy in 9 of 17 patients, and they required less cumulative rpFVIII for resolution of the presenting bleed compared with the 8 patients given rpFVIII as rescue therapy (first-line median cumulative dose = 300 U/kg, rescue median cumulative dose = 1400 U/kg, P = .0016; Figure 4A). This could not be explained by differences in BIA, since there was no difference in median preexposure pBIA in the first-line or second-line groups. (Figure 4B). Our observation of patients receiving rpFVIII as first-line therapy having better bleed control (measured as a lower cumulative dose for hemostasis) is consistent with a similar metric in the trial evaluating rpFVIII in AHA. That trial showed higher rates of bleed control when rpFVIII was used as first-line therapy vs second-line, 94% vs 73%.14 We also explored potential explanations of this difference in outcomes in our cohort.
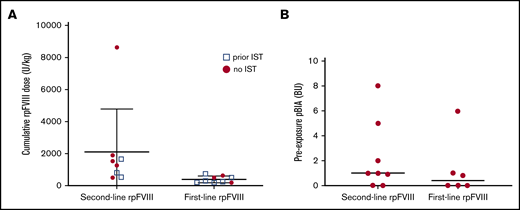
Comparison of therapy response in patients given rpFVIII as first-line vs second-line therapy as previously defined. When used as second-line therapy, more cumulative rpFVIII was required for bleed control in our cohort (see “Results” and “Discussion” for details). Median dose required for the second-line dosing was 1400 U/kg, and was, for upfront dosing, 300 U/kg with a P value of .0016 by Mann-Whitney U test. (A) Cumulative rpFVIII dose required for presenting bleed. (B) Preexposure pBIA in first-line and second-line groups. There was no significant difference in preexposure pBIA between those treated with rpFVIII as first line or second line by the same test.
Comparison of therapy response in patients given rpFVIII as first-line vs second-line therapy as previously defined. When used as second-line therapy, more cumulative rpFVIII was required for bleed control in our cohort (see “Results” and “Discussion” for details). Median dose required for the second-line dosing was 1400 U/kg, and was, for upfront dosing, 300 U/kg with a P value of .0016 by Mann-Whitney U test. (A) Cumulative rpFVIII dose required for presenting bleed. (B) Preexposure pBIA in first-line and second-line groups. There was no significant difference in preexposure pBIA between those treated with rpFVIII as first line or second line by the same test.
Bleeding severity was similar between groups receiving first-line vs second-line rpFVIII. Of the 9 patients treated with first-line rpFVIII, 7 had severe bleeding and 2 had CRNMB. Of the 8 patients treated as second-line, 7 had severe bleeding, and 1 had CRNMB. Of the 9 patients for whom a baseline Hb was known, 5 were treated with first-line rpFVIII and had a mean Hb decrease of 3.2 g/dL. Four were treated after failure of BPAs and had a mean Hb decrease of 3.6 g/dL (Table 2).
As compared with the initial trial evaluating rpFVIII in patients with AHA, we observed lower – yet still therapeutic – median first-dose recovery (117% vs 216%) and peak FVIII activity in the first 24 hours of therapy (139% vs 308%; Table 3).
Our patients required significantly less rpFVIII in the first 24 hours of therapy (220.6 U/kg vs 741.1 U/kg) and had lower cumulative dose requirement per patient for the bleed episode (1191 U/kg vs 2057 U/kg). We observed similar mean intervals between doses (9.6 vs 10.2 hours). While not surprising that we used lower cumulative doses (given our lower starting dose), this demonstrates that hemostasis can be effectively achieved with similar dosing intervals despite using these much lower doses by using an algorithm-based approach.
Because follow up pBIA titers were not monitored on a consistent schedule and some patients were subsequently lost to follow-up, we did not perform a systematic analysis of cumulative rpFVIII dose and subsequent peak pBIA.
Discussion
Given their excellent track record, BPAs are generally first line bleed treatments for patients with AHA. While some (including our center) advocate rpFVIII as first-line therapy, cost and availability of the product have limited adoption of this approach.25,26 Using a dosing algorithm that spares product use, while also allowing for close monitoring of efficacy, has changed our practice to preferentially using rpFVIII over BPAs.
We have previously reported effective bleed control using our algorithm in a 4-patient series,20 and this update validates the utility of this approach in a total of 18 patients with AHA. Only 1 patient did not have successful bleed control, and was given a single, attempted rescue dose of rpFVIII prior to transitioning to hospice.
Foremost among our findings from this cohort is the poor utility in preexposure pBIA. Clinical and laboratory response was poorly predicted by this value in our cohort and there was no major difference in the cumulative dose required for bleed control between those with a preexposure low- or high-titer pBIA (Figure 3). These findings support the use of an algorithm and rapid administration of rpFVIII, provided FVIII activity can be monitored via OSCA. If OSCA is not available within a meaningful time frame, there is less advantage to using rpFVIII. In the setting where FVIII activity can be rapidly monitored using OSCA, there is substantial benefit in using rpFVIII, both from an efficacy and monitoring standpoint. As discussed above regarding patients who did lose response, subsequent pBIA monitoring is useful, as a postexposure, high titer pBIA predicted loss of response in 5 of 7 such patients.
We have attempted to address confounding factors by providing granular, descriptive data for each patient. We indicated whether patients had received some sort of immunosuppression prior to receiving rpFVIII to illustrate that a subset of those who had rpFVIII as both first-line and second-line therapy had IST (Figure 4A). Although there were more patients who received IST in the first-line group, this discrepancy reflects the administration of rituximab prior to the first dose of rpFVIII in most cases. Although the number of patients on IST prior to receiving rpFVIII do not allow for meaningful statistical analysis, we observed patients with prior IST in both the first-line and rescue groups with a range of cumulative doses.
Both our data and trial data suggest that using rpFVIII as first-line therapy is more effective than as a second-line agent.1,14 In our cohort, receiving rpFVIII as second-line therapy after BPAs was associated with a need for a greater cumulative dose of rpFVIII to obtain for bleed control, even for clinically relevant non-major bleeding. All bleeding episodes treated with first-line rpFVIII in our cohort were well controlled, with only 1 failure in the second-line group. Our findings of much lower doses being efficacious provide additional rationale to use rpFVIII as first-line intervention, as long as appropriate laboratory monitoring can be performed. This may assuage cost concerns of using rpFVIII as first-line therapy. Superiority of first-line dosing at lower than FDA recommended doses has previously only been observed in patients with cHA.7-9 Observational, prospective cohorts have clear limitations, yet directly replacing the factor defect, as is the case with rpFVIII as opposed to BPAs, represents a different physiologic process.
Total cumulative dose was demonstrably lower for hemostatic control in our cohort, and more pronounced in the group who received first-line rpFVIII. While FDA dosing recommends titration based on troughs, dosing can be more rapidly weaned and spaced while remaining in therapeutic ranges using our algorithm. We observed clinical hemostasis in all cases when FVIII activity was at therapeutic levels as per our dosing algorithm (ie, we had no cases of in vitro normalization of FVIII activity without corresponding clinical response).
The ability to use first-line rpFVIII with real-time monitoring per our algorithm resulted in substantially lower product usage, which can lead to cost savings over standard dosing of BPAs. Due to the inability in some cases to account for all doses of BPAs given prior to transfer to our facility, we did not systematically analyze cost in our cohort. However, some cost-analysis data exist to infer potential cost savings. An economic analysis of AHA treatment reported rpFVIII costs as being comparable to using rFVIIa if factor utilization can be reduced by 50%, along with pharmacy cost reduction of 30%.27,28 Using the proposed algorithm, we have, on average, used ∼70% less rpFVIII in the first 24 hours, and 42% less cumulative product for initial bleed control as compared with recommended dosing in the phase 2/3 trial. This difference in cumulative product utilization for bleed treatment may greatly mitigate cost concerns for a treating institution.
While some patients lose response to rpFVIII, a clinical and financial concern in AHA care, this loss of response was variable and unpredictable. Extremely high hBIA titer was present in the individuals with poor initial response, and recent data have shown that cross-reacting inhibitors are more common in patients with very high hBIA, although that cross-reactivity is rare.29 Of our 2 patients with no initial response to rpFVIII, both had very high hBIA, with 1 patient having very high pBIA as well (186 BU), while the other had only a low-titer pBIA (2 BU). Of the 3 patients who developed a new pBIA following exposure (patients 2, 14, and 15), only 1 was observed to lose FVIII response to continued dosing. The other 4 who lost response had high-titer postexposure pBIA.
Important for management of bleeds in AHA, the presence of a porcine inhibitor (or increase in titer) in these patients did not impair the algorithm-directed approach, as patients showing cross reactivity or neutralizing anti-pFVIII antibodies can be quickly identified by their lack of response using OSCA. In our experience, laboratory response based on OSCA was much more quickly ascertained that awaiting pBIA results.
Administration of any therapy for bleeding is generally more effective the sooner it is able to be given.12 When AHA is suspected in the setting of severe bleeding, our evolving clinical practice is to administer 100 U/kg rpFVIII as first-line therapy, with monitoring according to the algorithm in Figure 1. We recommend such an approach at any institution capable of this degree of monitoring. Use of an algorithm that utilizes first-dose recovery as an initial decision point gives the clinician quantitative data within a short time period; this direct observation, in our experience, is more useful than knowing inhibitor titers.
Regarding FVIII activity assays, although we have both chromogenic and OSCA available at our institution, we use the OSCA for monitoring in rpFVIII treatment. This is preferable due to the available data showing that the chromogenic FVIII activity assay tends to underestimate FVIII activity as compared with the OSCA in these cases.3,16
Because therapeutic FVIII activity on OSCA is generally reflective of in vivo hemostasis, this approach not only leads to rapid hemostasis, but can reassure other consultants and colleagues of hemostatic potential should surgery or other procedures take place.
Recent data demonstrating good short-term effectiveness of rpFVIII have shown an increase in hBIA with administration of rpFVIII.26,29 We observed this in 7 of our 18 patients, but this did not impair the usefulness of our dosing algorithm, as we initiate IST in all patients at time of diagnosis. We did not systematically compare IST regimens, but there were not substantial differences between IST given to patients who did or did not lose response to rpFVIII. Discussion of inhibitor eradication is beyond the scope of this presentation but warrants mention as the uncertain trajectory of a large proportion of patients leaves reliable treatment of bleeds an important part of a care plan.
In conclusion, our data validate our previously established dosing algorithm, providing hemostatic efficacy at substantially lower than FDA-approved doses, while providing a monitoring mechanism that can quickly identify nonresponders and avoid excess product usage.
When using such an algorithm, clinicians can confidently administer rpFVIII as first-line therapy while awaiting the results of the preexposure pBIA, and quickly determine efficacy or lack of response. Subsequent titers can also be useful in case of repeat bleeding events after initial treatment. Although the pBIA is usually unknown at the time of presentation and at initiation of therapy, clinicians should not be dissuaded from using rpFVIII for that reason. Using the proposed algorithm has allowed providers and pharmacists to monitor FVIII levels closely and respond in a standardized way without delaying initial treatment. A consequence of this algorithm is that rpFVIII should only be administered in centers where FVIII activity via OSCA can be done in a fast and reliable manner.
In some cases, rpFVIII use with FVIII monitoring allows for substantial pharmacy cost savings over rVIIa or aPCCs, favoring first-line use. Easy monitoring of adequate dosing, as opposed to BPAs, allows for bleed control in patients with complicated comorbidities such as coronary artery disease or stroke who require antiplatelet therapy.30 In our cohort of patients, we observed no thrombotic complications related to the rpFVIII use. Given the simplicity of therapeutic monitoring, we would anticipate a low rate of thrombotic complications in general with use of rpFVIII.
Finally, our experience is ongoing with a growing cohort of patients. Our observations are prospective and have been useful in guiding therapy at our institution and should be able to be useful and able to be used at any institution with rapidly available FVIII activity in their laboratory.
Requests for data may be e-mailed to the corresponding author, Alice Ma, at alice_ma@med.unc.edu.
Acknowledgments
P.E. is a National Hemophilia Fellow and receives funding from the NHF-Takeda Clinical Fellowship Award program.
Authorship
Contribution: P.E. collected and analyzed data and wrote the manuscript; S.-L.C. collected and managed patient data; A.D.M. assisted with data analysis and manuscript preparation; and N.S.K., R.S.K., and M.J.M. provided patient data and assisted with editing the manuscript.
Conflict-of-interest disclosure: A.D.M. has received honoraria and research funding from Takeda (Shire). N.S.K. has received research funding from Shire. The remaining authors declare no competing financial interests.
Correspondence: Alice D. Ma, UNC Chapel Hill, Houpt Building, CB# 7305, 170 Manning Dr, 3rd Floor, Chapel Hill, NC 27599-7305; e-mail: alice_ma@med.unc.edu.