Key Points
Number of NAs used prior to alloHCT and NA immediately preceding alloHCT do not impact survival outcomes.
Hematopoietic cell transplantation-specific comorbidity index predicts PFS, yet PFS is not impacted by high-risk disease characteristics.

Abstract
Although novel agents (NAs) have improved outcomes for patients with chronic lymphocytic leukemia (CLL), a subset will progress through all available NAs. Understanding outcomes for potentially curative modalities including allogeneic hematopoietic stem cell transplantation (alloHCT) following NA therapy is critical while devising treatment sequences aimed at long-term disease control. In this multicenter, retrospective cohort study, we examined 65 patients with CLL who underwent alloHCT following exposure to ≥1 NA, including baseline disease and transplant characteristics, treatment preceding alloHCT, transplant outcomes, treatment following alloHCT, and survival outcomes. Univariable and multivariable analyses evaluated associations between pre-alloHCT factors and progression-free survival (PFS). Twenty-four-month PFS, overall survival (OS), nonrelapse mortality, and relapse incidence were 63%, 81%, 13%, and 27% among patients transplanted for CLL. Day +100 cumulative incidence of grade III-IV acute graft-vs-host disease (GVHD) was 24%; moderate-severe GVHD developed in 27%. Poor-risk disease characteristics, prior NA exposure, complete vs partial remission, and transplant characteristics were not independently associated with PFS. Hematopoietic cell transplantation–specific comorbidity index independently predicts PFS. PFS and OS were not impacted by having received NAs vs both NAs and chemoimmunotherapy, 1 vs ≥2 NAs, or ibrutinib vs venetoclax as the line of therapy immediately pre-alloHCT. AlloHCT remains a viable long-term disease control strategy that overcomes adverse CLL characteristics. Prior NAs do not appear to impact the safety of alloHCT, and survival outcomes are similar regardless of number of NAs received, prior chemoimmunotherapy exposure, or NA immediately preceding alloHCT. Decisions about proceeding to alloHCT should consider comorbidities and anticipated response to remaining therapeutic options.
Introduction
Prior to the availability of targeted novel agents (NAs) in clinical practice, consideration of allogeneic hematopoietic stem cell transplantation (alloHCT) was recommended for patients with poor-risk chronic lymphocytic leukemia (CLL), specifically those with early relapse or refractory disease after purine analog based treatment or those with TP53 aberration.1 For these poor-risk patients, alloHCT represented an opportunity for long-term disease control in the absence of other effective therapies, and subsequent retrospective analyses suggested a survival advantage of alloHCT.2-8
B-cell receptor inhibitors (BCRi’s) including Bruton tyrosine kinase inhibitors (BTKi’s; ibrutinib and acalabrutinib) and phosphoinositide 3-kinase inhibitors (PI3Ki; idelalisib and duvelisib), as well as the BCL2 inhibitor (BCL2i) venetoclax have fundamentally changed the treatment landscape of CLL and natural history of the disease. These drugs have improved response rates, progression-free survival (PFS), and overall survival (OS), including in patients with high-risk disease.9-24 AlloHCT carries risks including graft-versus-host disease (GVHD), organ toxicity, and nonrelapse mortality (NRM); in light of the potential for long-term disease control with sequential administration of NAs, the necessity of pursuing long-term disease control with alloHCT is less defined.25
Despite effective NAs, drug intolerance, progression, primary resistance, and high-grade transformation remain as serious limitations for many patients. For patients who experience progression or toxicity on all of the available NAs, outcomes remain poor.26-29 Therefore, the optimal timing of alloHCT within the sequence of NAs is an important unanswered question.30-33 Given the paucity of data regarding alloHCT experience in the era of NAs and the near absence of data-driven consensus regarding role of alloHCT for CLL, the decision about proceeding to alloHCT is currently based on disease and alloHCT risk, response to NA, donor availability, and patient preference. As a result of patient selection and timing of alloHCT, the patient population undergoing alloHCT following NA therapy may be quite different from those reported in previous series based on disease biology, number of prior lines of therapy, or baseline immunosuppression from chemoimmunotherapy vs NA exposure. Here, we aim to describe an NA-exposed population of patients who have undergone alloHCT in order to help define the role of alloHCT in CLL in the contemporary era.
Methods
Patient population
We conducted an international, multicenter, retrospective cohort study to examine adult patients with CLL or small lymphocytic lymphoma (SLL) who were treated with NAs prior to undergoing alloHCT. Patients were included if they had received at least 1 NA (BTKi, PI3Ki, or BCL2i) as CLL-directed therapy prior to the date of their alloHCT. All graft and donor types, as well as all conditioning regimens, were included. Patients with Richter transformation prior to alloHSCT were excluded. The study was approved at each participating center by an institutional review board.
We collected patient and disease-related characteristics, prior lines of therapy, transplant characteristics and outcomes, and therapy following alloHCT for patients who experience disease progression. Patient characteristics included age at CLL diagnosis and alloHCT, sex, race, and calculated the hematopoietic cell transplantation–specific comorbidity index (HCT-CI).34 Pre-alloHCT disease-related characteristics included cytogenetics (deletion of chromosome 11q [del11q], deletion of chromosome 17p [del17p], complex karyotype [CK; ≥3 chromosomal abnormalities35 ]), IGHV mutational status, disease burden (elevation of lactate dehydrogenase [LDH] or β-2 microglobulin). For each line of therapy prior to alloHCT, response, time from therapy initiation to progression or next therapy, and reason for discontinuation were collected. International Workshop on CLL (iwCLL) guidelines were used to define response to CLL-directed therapies, including complete remission (CR), partial remission (PR), stable disease (SD), and progressive disease (PD).35 For patients who achieved CR or PR, we additionally collected whether patients had been tested for or achieved undetectable minimal residual disease (MRD; U-MRD) with a suggested sensitivity ≤10−4. Transplant characteristics collected included donor source and HLA match, conditioning intensity,36,37 GVHD prophylaxis regimen, and cytomegalovirus (CMV) status of patients and donors. Transplant outcomes included development of GVHD, occurrence and timing of progression, relapse, NRM, and death.
The primary objective was to describe PFS of patients undergoing alloHCT who had received an NA prior to alloHCT. Secondary objectives included determination of OS, NRM, and relapse. Data cutoff was 15 July 2019.
Statistical analysis
PFS and OS were estimated with the Kaplan-Meier method.38 PFS was defined as the time elapsed from alloHCT to PD or death from any cause. OS was defined as the time from alloHCT to death from any cause. NRM probability was estimated using cumulative incidence with relapse or PD as competing events. Relapse and acute GVHD (grades II-IV and III-IV) were estimated using cumulative incidence with death as a competing event.
Using Cox regression, we conducted univariable and multivariable analyses evaluating the association between pre- alloHCT disease/treatment-related characteristics and PFS. Del11q, del17p, CK, TP53 mutational status, disease response at time of alloHCT (CR vs PR), HCT-CI (stratified 0 vs ≥1), donor type, CMV seropositivity, and exposure to prior therapies were analyzed as categorical variables. Analysis of exposure to prior therapies included use of ibrutinib, venetoclax, or PI3Ki in any line of therapy prior to alloHCT, as well as use of 2 or more NAs as any line of therapy prior to alloHCT. Additionally, patients were categorized based on having received exclusively NAs prior to alloHCT vs NA and chemo/chemoimmunotherapy as sequential lines of therapy before alloHCT. For patients who had received chemotherapy or chemoimmunotherapy combinations, the first line of chemoimmunotherapy was considered, and patients were classified as refractory35 vs responsive. HCT-CI was additionally analyzed as a continuous variable in univariable analysis. For all variables, hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated for association with PFS using Cox regression. Categorical variables associated with PFS to a level of P < .05 in univariable analysis were included in multivariable analysis. Statistical analyses were performed using STATA 10.1 (Stata statistical software: Release 10, 2007; StatCorp LP, College Station, TX).
Results
Baseline and transplant characteristics
Across 6 US and 9 European centers, we identified 65 patients with CLL/SLL who underwent alloHCT after treatment with at least 1 NA. All patients were NA exposed, though not necessarily refractory to NAs. Baseline and transplant characteristics are described in Table 1.
Therapy prior to alloHCT
Prior to alloHCT, patients had received a median of 3 lines of therapy (range, 1-9) and 1 NA (range, 1-3). Twenty-nine percent (18 of 63) had exclusively received NAs as CLL-directed therapy prior to alloHCT. The 3 most common NAs used in any line of therapy prior to alloHCT were ibrutinib for 82% (53 of 65), venetoclax for 40% (26 of 65), and idelalisib for 20% (13 of 65) (Table 2). Twenty-six percent (17 of 65) had received both ibrutinib and venetoclax. Chemoimmunotherapy was given in any line of therapy prior to alloHCT in 71% (45 of 63). In patients for whom response assessment to chemoimmunotherapy was available, 27% (9 of 33) were refractory to their first chemoimmunotherapy regimen.
Ninety-two percent (60 of 65) received an NA immediately prior to alloHCT. Of these 60 patients, 33 were treated with ibrutinib with median time on therapy of 9 months (range, 2-35 months). Fifty percent (16 of 32) had TP53 aberrations and 46% (11 of 24) had CK. Best response to ibrutinib was CR in 6% (2 of 32), PR or PR with lymphocytosis in 91% (29 of 32), and SD in 3% (1 of 32). Of these patients, 97% (32 of 33) discontinued ibrutinib to proceed to a planned alloHCT whereas a single patient discontinued for PD. Twenty-three patients were treated with venetoclax-based therapy immediately prior to alloHCT with best response of CR in 52% (11 of 21), PR in 43% (9 of 21) PR, and SD in 5% (1 of 21). Fifty-six percent (10 of 18) had TP53 aberrations and 36% (5 of 14) had CK. Venetoclax discontinuation occurred for planned alloHCT in 95% (20 of 21) and intolerance in 5% (1 of 21). Four patients received PI3Ki (all idelalisib) immediately prior to alloHCT, all achieving PR. Idelalisib was discontinued for planned alloHCT in 3 patients and progression of disease in 1 patient.
Efficacy
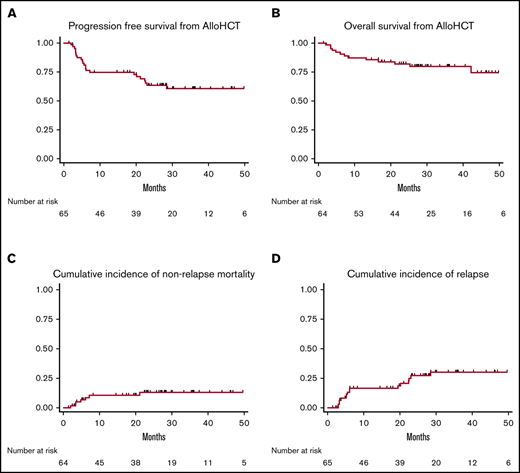
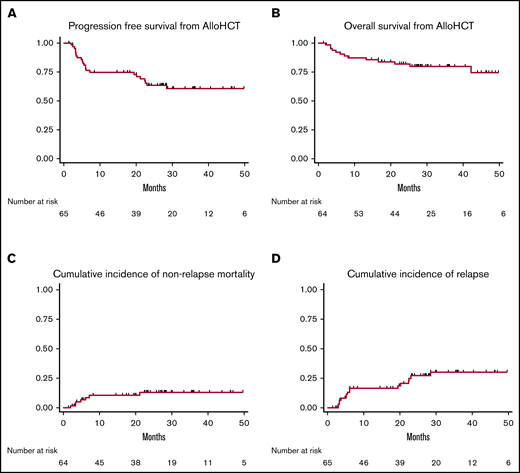
Median PFS and OS were not reached after a median follow-up of 27 months (range, 1.2-85 months) for the entire cohort, 29 months for survivors from time of alloHSCT. PFS was estimated to be 75% (95% CI, 62% to 84%) at 12 months and 63% (95% CI, 50% to 74%) at 24 months. OS was estimated to be 85% (95% CI, 74% to 92%) at 12 months and 81% (95% CI, 70% to 90%) at 24 months. NRM was 5.1% (95% CI, 2% to 15%) at day +100, 11% (95% CI, 5% to 22%) at 12 months, and 13% (95% CI, 6% to 26%) at 24 months. Relapse incidence was 8.1% (95% CI, 3% to 18%) at day +100, 17% (95% CI, 9% to 29%) at 12 months, and 27% (95% CI, 17% to 41%) at 24 months (Figure 1). At day +100, cumulative incidence of grade II-IV acute GVHD was 37% and grade III-IV acute GVHD was 24%. Moderate to severe chronic GVHD occurred in 27% (17 of 62).39

Outcomes for all patients with CLL from time of alloHCT. (A) PFS. (B) OS. (C) Cumulative incidence of NRM. (D) Cumulative incidence of relapse.
Outcomes for all patients with CLL from time of alloHCT. (A) PFS. (B) OS. (C) Cumulative incidence of NRM. (D) Cumulative incidence of relapse.
Thirteen of 65 patients who underwent alloHCT for CLL have died. Six patients experienced PD prior to death; the cause of death for the remaining 7 patients was infection in 6 and GVHD in 1. A total of 16 patients have experienced disease relapse, of whom 15 have required CLL-directed therapy following alloHCT; the line of therapy immediately following relapse was venetoclax (n = 5; 3 had received venetoclax prior to alloHCT), ibrutinib (n = 4; 3 had received ibrutinib prior to alloHCT), rituximab (n = 2), R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) (n = 1), R-HyperCVAD (rituximab, fractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone) (n = 1), duvelisib (n = 1), and second alloHCT (n = 1).
Predictors of PFS
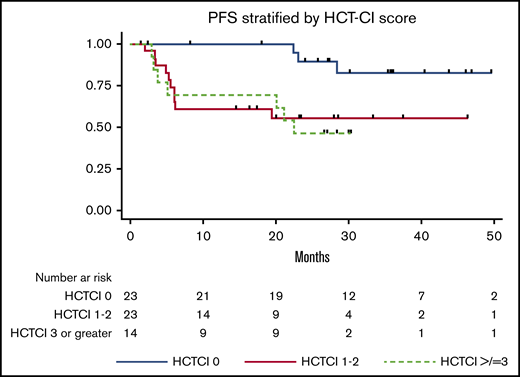
Poor risk disease characteristics (TP53 mutation, del17p, del11q, CK), depth of response in those with responding disease (PR vs CR), patterns of prior NA exposure (ibrutinib, venetoclax, PI3Ki, ≥2 NAs, exclusive therapy with NAs, and NA immediately preceding alloHCT), disease refractory to first line of chemotherapy, and transplant characteristics (8 of 8 matched vs mismatched donor, patient positive/donor negative vs other CMV serology) were not associated with inferior PFS in univariable analyses. HCT-CI (≥1 vs 0; HR 3.9; 95% CI, 1.3-11.5; P = .015) and donor source (related vs unrelated; HR, 2.7; 95% CI, 1.2-6.4; P = .019) were significantly associated with PFS in univariable analyses (Table 3). In multivariable analysis, HCT-CI score of ≥1 (vs 0; HR, 3.3; 95% CI, 1.1-9.9; P = .035) remained independently associated with inferior PFS. Figure 2 depicts PFS stratified by HCT-CI score.

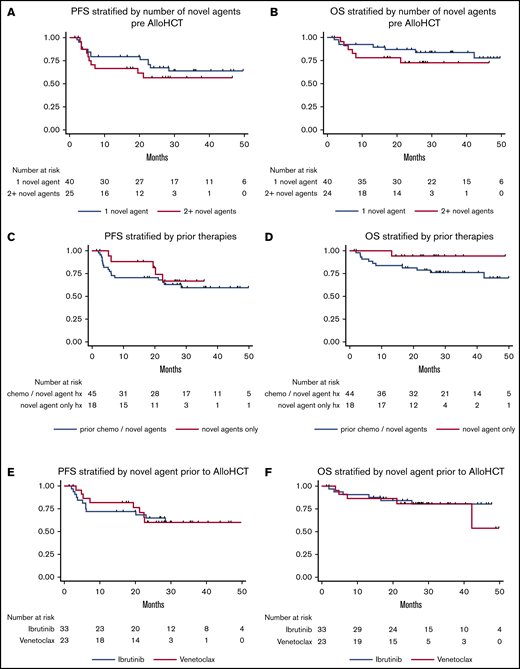
We examined patients who had received 1 (n = 40) vs ≥2 (n = 25) NAs prior to alloHCT and found that PFS and OS were not significantly different for these groups (Figure 3A-B). These groups were similar in terms of poor-risk features including del17p (51% vs 33%; P = .17), TP53 mutation (59% vs 39%; P = .18), and CK (50% for both groups). These groups were similar in terms of age at alloHCT (median 60 for both groups), HCT-CI score (median 0 vs 1), and proportion who had a matched donor (88% vs 75%). Of those who received 1 NA, the therapy immediately preceding alloHCT was ibrutinib for 73% (29 of 40), venetoclax for 10% (4 of 40), anti-CD20 monoclonal antibody for 7.5% (3 of 40), idelalisib for 5% (2 of 40), chemoimmunotherapy for 5% (2 of 40), and other for 2.5% (1 of 40). Among those who received ≥2 NA, the therapy immediately preceding alloHCT was venetoclax for 76% (19 of 25), ibrutinib for 16% (4 of 25), and PI3Ki for 8% (2 of 25). Seventeen patients have received both ibrutinib and venetoclax. Of these 17, 82% (14 of 17) had experienced progression of disease on 1 agent, and 2 patients experienced progression of disease on both agents.
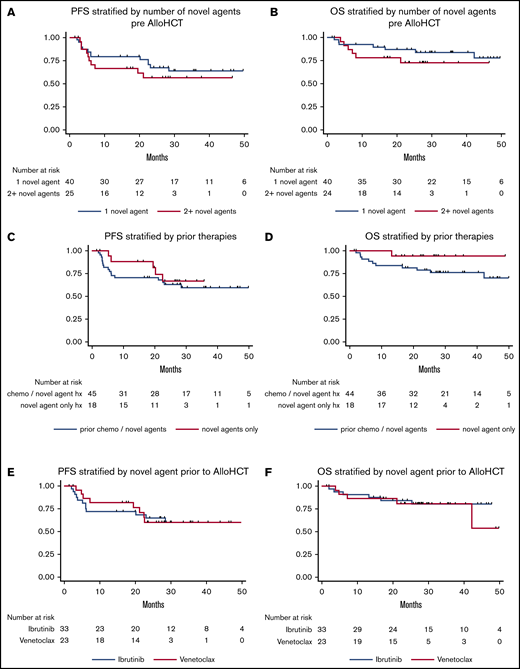
Survival outcomes for all patients with CLL from time of alloHCT. (A) PFS stratified by number of prior NAs. (B) OS stratified by number of prior NAs. (C) PFS stratified by those who had only received NAs vs those who had received chemotherapy and NAs as lines of therapy prior to transplant. (D) OS stratified by those who had only received NAs vs those who had received chemotherapy and NAs as lines of therapy prior to transplant. (E) PFS stratified by NA received immediately prior to alloHCT, ibrutinib vs venetoclax. (F) OS stratified by NA received immediately prior to alloHCT, ibrutinib vs venetoclax.
Survival outcomes for all patients with CLL from time of alloHCT. (A) PFS stratified by number of prior NAs. (B) OS stratified by number of prior NAs. (C) PFS stratified by those who had only received NAs vs those who had received chemotherapy and NAs as lines of therapy prior to transplant. (D) OS stratified by those who had only received NAs vs those who had received chemotherapy and NAs as lines of therapy prior to transplant. (E) PFS stratified by NA received immediately prior to alloHCT, ibrutinib vs venetoclax. (F) OS stratified by NA received immediately prior to alloHCT, ibrutinib vs venetoclax.
For the 18 patients who had exclusively received NAs (“chemotherapy free”) prior to alloHCT, the median number of lines of therapy prior to alloHCT was 2 (range, 1-3) and median NAs received was 1.5 (range, 1-2) with 72% (13 of 18) receiving ibrutinib, 56% (10 of 18) receiving venetoclax, and 22% (4 of 18) receiving PI3Ki. TP53 aberrations were detected in 75% (12 of 16) with del17p in 53% (8 of 15) and TP53 mutations in 57% (8 of 14). Fifty percent (6 of 12) had CK. In this group, median PFS and OS were not reached with median follow up of 26.4 months among survivors (range, 2.0-53.9 months). Twenty-four-month PFS was estimated at 66% (95% CI, 37% to 85%) and OS was 94% (95% CI, 65% to 99%). NRM at 24 months for this group was 0%. PFS and OS were not significantly different for chemotherapy-free patients compared with those who received chemotherapy and NAs as pre-alloHCT lines of therapy (Figure 3C-D).
Finally, we examined patients who underwent alloHCT for CLL who had received ibrutinib (n = 33) vs venetoclax (n = 23) as the NA immediately preceding alloHCT. The median number of lines of therapy prior to alloHCT was 3 for both groups. Of the 33 who received ibrutinib as the line of therapy prior to alloHCT, 2 had prior venetoclax exposure and both had disease progression on venetoclax. Of the 23 who received venetoclax immediately prior to alloHCT, 15 had prior ibrutinib exposure. CLL status at time of alloHCT for those who received ibrutinib vs venetoclax was CR 12% (4 of 33) vs 48% (11 of 23), PR 79% (26 of 33) vs 43% (10 of 23), SD/PD 9% (3 of 33) vs 9% (2 of 23). No differences in PFS or OS were observed between the 2 groups. 12-month relapse incidence was 20% in the ibrutinib cohort and 9.3% for the venetoclax cohort.
Discussion
As NAs have transformed the management CLL/SLL, the number of alloHCTs performed for CLL has steadily declined with a 58% decrease in number of alloHCTs performed from 2010 to 2018 in the United States.40 As much of the prospective research on cellular immunotherapy has shifted to focus on chimeric antigen receptor T cells (CAR-T), multicenter experiences illustrating outcomes for those undergoing alloHCT following therapy with NAs are needed to help inform the role of this cellular immunotherapy, with the potential for curative intent, in future practice. In this study, we describe a multicenter, international cohort of 65 patients with CLL who underwent alloHCT following exposure to ≥1 NAs and notably include patients who have received venetoclax prior to alloHCT.
Although NAs have induced durable responses and prolonged survival, a subset of patients will eventually have disease progression through all available NAs. Further, there is a group of high-risk patients in whom PFS and OS with NAs are likely inferior compared with those patients without these features (ie, del17p, TP53 mutation, CK). The data presented here support consideration of alloHCT for NA treated, fit patients, with responding disease and should be considered particularly for patients in whom NAs are not expected to provide long-term disease control.
In this cohort, NRM, PFS, and OS at 24 months following alloHCT were 14%, 60%, and 80%, respectively. Prospective CLL-specific trials examining reduced intensity conditioning alloHCT prior to the introduction of NAs for CLL include CLL3X, which showed 2-year NRM, EFS, and OS of 18%, 50%, and 75%,41 as well as a Cooperative German Transplant Study Group which reported a 2-year PFS and OS of 67% and 72%.42 In large retrospective studies, reported 2-year OS have ranged from 51% to 72% and PFS 34% to 56%.2,43-48
Although the extent of the difference in disease biology and immunocompetence after NA exposure as compared with chemotherapy is unclear, the outcomes observed in our cohort are comparable to prospective and retrospective studies of CLL alloHCT prior to the introduction of NA. Considering the relatively low incidence of acute GVHD, chronic GVHD, and NRM, we observed, it appears that the use of NA in the sequence of therapies prior to alloHCT does not negatively impact alloHCT safety in this patient population. The low observed NRM relative to older studies of reduced intensity conditioning alloHCT is likely a testament to the ongoing refinement of transplantation technique and supportive care.49,50 Further, we describe a small series of CLL patients who had no exposure to cytotoxic chemotherapy for CLL management and then underwent alloHSCT. This series demonstrates comparable outcomes for those with and without prior chemotherapy exposure (PFS: HR, 0.59; 95% CI, 0.22-1.6; P = .29), providing some reassurance for use of this modality in a disease increasingly managed exclusively with NAs.
The number of NAs received prior to alloHCT did not significantly impact PFS or OS in this study. Although this observation might suggest that alloHCT can be deferred to later lines of therapy without affecting outcomes, it must be considered that successive lines of therapy are associated with lower response rates and risk of treatment related toxicities, meaning that a proportion of patients may die or become unfit before entering the next line of therapy, including alloHCT.22,51-53 Furthermore, most patients had responsive disease at the time of transplant in this cohort, thus conclusions regarding use of alloHCT in the setting of disease progression cannot be drawn from this study. With this in mind, determining the optimal timing of alloHCT needs to be carefully considered.
As a hypothesis generating exercise to explore the optimal bridging strategy, we examined those who received ibrutinib vs venetoclax as their line of therapy immediately preceding alloHCT. No significant differences in PFS or OS were observed between these groups. Although the number of patient and events in each group is small, 12-month relapse incidence was 20% for ibrutinib-bridged patients vs 9% for venetoclax-bridged patients. A prior report of ibrutinib treated CLL and mantle cell lymphoma patients undergoing alloHCT reported a 12-month relapse incidence of 30%, which was higher than prior series of non-ibrutinib exposed patients. It has been hypothesized that responses to ibrutinib were less durable after drug withdrawal, precluding sufficient disease control until graft-versus-leukemia (GVL) effect was established.54 As venetoclax more frequently induces deeper remissions leading to durable responses after withdrawal,23,24 it is possible that patients bridged to alloHCT with venetoclax may experience fewer early relapses. Further study on the optimal bridging strategy to alloHCT is warranted.
American Society for Blood and Marrow Transplantation (ASBMT) clinical practice recommendations suggest alloHCT for standard risk patients refractory to BCRi and for TP53 aberrant or CK patients following failure of 2 lines of therapy with response to BCRi.33 Updated recommendations from the European Society for Blood and Marrow Transplantation (EBMT) and European Research Initiative on CLL (ERIC) suggest dividing high-risk CLL into 2 categories: those with chemoimmunotherapy-resistant disease with TP53 aberrations but response to NAs defined as high-risk I, and those who are resistant to chemoimmunotherapy and at least 1 NA defined as high-risk II.32 For the high-risk I category, cellular immunotherapy is recommended only for patients with low cellular immunotherapy risk (age <65 years, absence of comorbidities, available well-matched donor). For the high-risk II category patients, cellular immunotherapy is recommended also for patients with higher transplant risk. Preliminary evidence suggests that this algorithm may be feasible.55
Our data support current guidelines. First, use of alloHCT for patients with high-risk disease is reasonable as alloHCT appears to overcome poor-risk genetic features including TP53 aberrations and CK, consistent with prior reports.2,6 A significant predictor of outcome in this series is HCT-CI, which reinforces the EBMT/ERIC recommendation that risk of cellular immunotherapy, including age, comorbidities, and donor availability, be a primary consideration for patients considering alloHCT. Our data additionally suggest that alloHCT can be pursued when patients are responding to therapy regardless of depth of response (CR vs PR), as PFS is not significantly different for these groups. It is also notable that these recommendations consider the potential for use of anti-CD19 CAR-T cells. CAR-T trials have demonstrated sustained remissions in heavily pretreated patients with relapsed/refractory CLL with overall response rates ranging from 38% to 74%,56-58 Although results are certainly promising with a subset of patients achieving deep responses and durable remissions, CAR-T is not yet widely available for CLL patients, has not been prospectively compared directly to alloHCT and is therefore still considered experimental without approved CAR-T products in CLL.
Notably, current recommendations largely focus on chemoimmunotherapy-resistant patients. As chemoimmunotherapy is less commonly used, fewer patients will be captured by these recommendations. Given increasing numbers of patients will be treated exclusively with NAs through several lines of treatment, considering alloHCT for patients receiving second-line NA therapy (regardless of prior chemoimmunotherapy exposure or depth of response in those with responding disease) seems to be warranted.
This study has several limitations, including its retrospective design, relatively small sample size, and heterogeneity of alloHCT strategies. Given the limited number of progression events in this cohort, evaluation of associations between disease or transplant characteristics and PFS may be underpowered to detect true associations. We were not able to assess whether patients with CK with ≥5 cytogenetic abnormalities have inferior PFS, as has been suggested in recent series.59 Investigators were asked to use iwCLL response criteria when reporting response to lines of therapy prior to alloHCT and disease status at time of alloHCT, though central review of this data were not performed. As expected in clinical practice, objective measures of response including CT imaging and bone marrow biopsy were not uniformly available. Further, MRD status at time of transplant was not uniformly collected, and the role of MRD status when considering cellular immunotherapy remains unclear. Monitoring for progression following alloHCT was not uniform across providers and centers, and progression events may have been subject to ascertainment bias. This cohort underwent alloHCT at large academic settings, and outcomes may not be wholly representative of all patients undergoing alloHCT for CLL.60 Although we describe a subset population of patients who had only received NAs, this group is small. As progression of disease through multiple NAs without prior chemotherapy exposure is going to represent an increasingly common clinical scenario, understanding outcomes for this population will become even more crucial.
Taken together, this study suggests that alloHCT is safe and effective in patients with CLL exposed to 1 or more NAs prior to alloHCT. These data support the use of alloHCT for well-selected patients with high-risk CLL. Decisions about proceeding to alloHCT should consider comorbidities and availability of clinical trials investigating alternative cellular therapeutic approaches including CAR-T. Particularly for young patients without comorbidities, consideration of alloHCT when prior NAs have failed and current NAs are inducing response is warranted. As the efficacy of NAs and the safety of alloHCT improve contemporaneously, updated prospective and real-world series will further inform the role of alloHCT in patients with CLL.
Data-sharing requests may be e-mailed to the corresponding author, Lindsey E. Roeker, at roekerl@mskcc.org. Data from patients have not been previously reported.
Acknowledgments
This work was supported in part by National Institutes of Health/National Cancer Institute Cancer Center support grant P30 CA008748 and Program Project grant P01 CA023766. T.A.E. received minor funding support from the National Institute for Health Research (NIHR) Biomedical Research Centre, based at Oxford University Hospitals Trust, Oxford, United Kingdom.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
L.E.R. has received an American Society of Hematology (ASH) Research Training Award for Fellows for work outside of this manuscript.
Authorship
Contribution: L.E.R. and A.R.M. designed the study with critical contributions from P.D., J.R.B., O.B.L., T.A.E., C.S.S., S.A.G., and M.-A.P.; L.E.R., P.D., J.R.B., O.B.L., T.A.E., D.M.B., A. Skarbnik, C.C.C., H.T.K., S.T.M., G.G., N.S., T.J.V., K.H.O., H.S.W., A.K.A., A. Sitlinger, C.S.S., and A.R.M. coordinated and collected data; L.E.R., P.D., J.R.B., T.A.E., C.S.S., and A.R.M. wrote the manuscript; and all authors contributed to the final manuscript.
Conflict-of-interest disclosure: L.E.R. has equity ownership in AbbVie and Abbott Laboratories. P.D. provided consultancy services to AbbVie, AstraZeneca, Gilead, Janssen, Novartis, Riemser, and Roche; was on speakers’ bureaus for AbbVie, Gilead, Novartis, Riemser, and Roche; held membership on an entity’s board of directors or advisory committees for, had symposia sponsored by, Merck Sharp & Dohme (MSD); and received research funding from Neovii and Riemser. J.R.B. provided consultancy services to TG Therapeutics, Octapharma, Dynamo Therapeutics, Sunesis, Juno/Celgene, Genentech/Roche, Catapult Therapeutics, AbbVie, Acerta Pharma, AstraZeneca, BeiGene, Novartis, Pfizer, and Pharmacyclics; provided consultancy services to and received research funding from Verastem, Gilead, Loxo, and Kite, a Gilead Company; received research funding from Sun Pharmaceuticals; received honoraria from Janssen and Teva; and was on data safety monitoring boards for Morphosys and Invectys. T.A.E. received honoraria from Roche; received honoraria from and traveled to conferences for AbbVie and Janssen; traveled to conferences for Takeda; and provided consultancy services to, received research support from, and was on a speakers’ bureau for Gilead. D.M.B. provided consultancy services to, and received honoraria and research funding from AbbVie, Genentech, and TG Therapeutics; provided consultancy services to and received honoraria from Teva; received research funding from Tolero, Acerta, BeiGene, DTRM Biopharma, and MEI; provided consultancy services to and received research funding from AstraZeneca; provided consultancy services to Novartis and Pharmacyclics LLC, an AbbVie Company; was a consultant to, served on a scientific advisory board of, and was site principal investigator (PI) on a clinical trial (grant paid to institution) for AbbVie, Verastem, and Genentech; was on a scientific advisory board for and was a site PI on a clinical trial (grant paid to institution) for ArQule and TG Therapeutics; was site PI on a clinical trial (grant paid to institution) for Ascentage, BeiGene, DTRM, Juno/Celgene/Bristol-Myers Squibb (BMS), MEI Pharma, and Tolero; was a consultant to and was a site PI on a clinical trial (grant paid to institution)for AstraZeneca and Pharmacyclics; was a consultant to and served on a scientific advisory board of Pfizer; was a consultant for Teva; held other guidelines/registry memberships (when sponsored or consultant also included under sponsor above): was a National Comprehensive Cancer Network (NCCN) panel member, and was on the informCLL registry steering committee (AbbVie), the REAL registry steering committee (Verastem), and the Biosimilars outcomes research panel (Pfizer). A. Skarbnik provided consultancy services to, received honoraria from, held membership on an entity’s board of directors or advisory committees, and was on a speakers’ bureau for AbbVie and Pharmacyclics; provided consultancy services to, received honoraria and research funding from, was on a speakers’ bureau for Janssen; received honoraria and research funding from, and was on a speakers’ bureau for Verastem Oncology; received honoraria from and was on speakers’ bureaus for Kite Pharma and Genentech; received honoraria from, held membership on an entity’s board of directors or advisory committees, and was on a speakers’ bureau for Gilead Sciences and Seattle Genetics; provided consultancy services to, received honoraria from, and was on a speakers’ bureau for Celgene; received research funding from Acerta; provided consultancy services to, held membership on an entity’s board of directors or advisory committees for the CLL Society; and was on speakers’ bureaus for Jazz Pharmaceuticals and Novartis. C.C.C. received research funding from H3 Biomedicine. M.D. provided consultancy services to AbbVie, AstraZeneca, Genentech, Janssen, MEI, Pharmacyclics, Syros Pharmaceuticals, and Verastem; received research funding from Acerta Pharma, Ascentage Pharma, Genentech, MEI pharma, Pharmacyclics, Surface Oncology, TG Therapeutics, and Verastem; received honoraria from Research to Practice; and held membership on an entity’s board of directors or advisory committees for AbbVie, Acerta Pharma, Adaptive Biotechnologies, AstraZeneca, Genentech, Gilead Sciences, Janssen, Pharmacyclics, and TG Therapeutics. N.S. received honoraria and/or travel support from Incyte, Celgene, and Miltenyi Biotec; served on scientific advisory boards for Kite, Celgene, Lily, TG Therapeutics, and Cellectar; has equity ownership in Exelixis, Oncosec, and Geron; and provided institutional research support for clinical trials to BMS and Miltenyi Biotec. K.H.O. held membership on an entity’s board of directors or advisory committees for Pfizer and Jazz Pharma; held membership on an entity’s board of directors or advisory committees for and received an unrestricted educational award for regional meetings from Gilead; and received unrestricted educational awards for regional meetings from Incyte and Adienne. J.H.P. provided consultancy services to Allogene, Amgen, AstraZeneca, Autolus, GlaxoSmithKline (GSK), Incyte, Intelllia, Kite Pharma, Novartis, Servier, and Takeda; served on a scientific advisory board of Artiva; and received research funding from Genentech, Servier, Autolus, Takeda, Incyte, and Fate Therapeutics. M.B.G. received research funding from Amgen. A.D.Z. received research grants from AbbVie, Adaptive Biotechnologies, BMS, BeiGene, Genentech/Roche, and MEI Pharma; received consulting fees from Amgen, AstraZeneca, BeiGene, Genentech/Roche, Janssen, JUNO/Celgene/BMS, Kite/Gilead, MEI Pharma, Pfizer, Pharmacyclics, and Sandoz/Novartis; and served on the scientific advisory board of Adaptive Biotechnologies and the Lymphoma Research Foundation. C.S.S. provided consultancy services to and received research funding from Juno Therapeutics, Sanofi-Genzyme, Celgene, and Precision Biosciences; received research funding from Bristol-Myers Squibb; and provided consultancy services to Spectrum Pharmaceuticals, Novartis, Kite/Gilead, Precision Biosciences, Genmab, Gamida Cell, and GSK. S.A.G. provided consultancy services to and received research funding from Johnson & Johnson, Amgen, Actinium, Takeda, and Celgene; provided consultancy services to Jazz Pharmaceuticals, Kite, Novartis, and Spectrum Pharmaceuticals; and received research funding from Miltenyi Biotec. M.-A.P. received honoraria from and held membership on an entity’s board of directors or advisory committees for Novartis, BMS, Omeros, Takeda, Nektar Therapeutics, Bellicum, and AbbVie; received honoraria from, held membership on an entity’s board of directors or advisory committees for, and received research funding from Incyte; provided consultancy services to and received honoraria from Merck; held membership on an entity’s board of directors or advisory committees for Medigene, Servier, NexImmune, MolMed, Cidara Therapeutics, and MolMed; received research funding from Kyte/Gilead and Miltenyi Biotec; received honoraria from Celgene; and serves in a volunteer capacity as a member of the Board of Directors of the American Society for Transplantation and Cellular Therapy (ASTCT) and Be The Match (National Marrow Donor Program [NMDP]), as well as on the Center for International Blood and Marrow Transplant Research (CIBMTR) Cellular Immunotherapy Data Resource (CIDR) Committee. A.R.M. provided consultancy services to Celgene; Acerta, Janssen, and Morphosis; provided consultancy services to and received research funding from AbbVie, LOXO, Genentech, Pharmacyclics, AstraZeneca, Sunesis, Johnson & Johnson, and Adaptive Biotechnologies; provided consultancy services to, was a member of the data safety monitoring board of, and received research funding from TG Therapeutics; and received research funding from DTRM Biopharma and Gilead. The remaining authors declare no competing financial interests.
Correspondence: Lindsey E. Roeker, Memorial Sloan Kettering Cancer Center, 1275 York Ave, New York, NY 10065; e-mail: roekerl@mskcc.org.