

¶ Martin-Rojas RM and Oarbeascoa G contributed equally to this work.
INTRODUCTION
Relapse is the main cause of treatment failure after allogeneic hematopoietic stem cell transplantation (allo-HSCT) for acute myeloid leukemia (AML). The evaluation of minimal residual disease (MRD) could provide a more accurate assessment of the depth of response, and therefore identify patients with higher risk of relapse.
AIMS
The aim of our study was to analyze the impact of pre-HSCT flow cytometry (FCM) and molecular MRD together with chimerism and MRD in the early post-HSCT period in patients with AML.
METHODS
We conducted a retrospective study in patients with complete remission AML who underwent a HSCT between 2008 and 2019 in our center. MRD was analyzed by flow cytometry in bone marrow aspirates and by quantitative RT-PCR (NMP1, RUNX1-RUNX1T1, CBFB-MYH11, KMT2A-MLLT3, WT1) in bone marrow aspirates and/or peripheral blood. MRD was determined within the 30 days preceding the HSCT and at day +30 and +90 post-HSCT. Bone marrow and selected CD34+ lineage chimerism was analyzed by STR (AmpFISTR SGM Plus, Thermo Fisher) at days +30 and +90 post-HSCT. This study was approved by our Institutional Ethics Committee. Data were analyzed using IBM SPSS Statistics version 24 and R version 3.5.1.
RESULTS
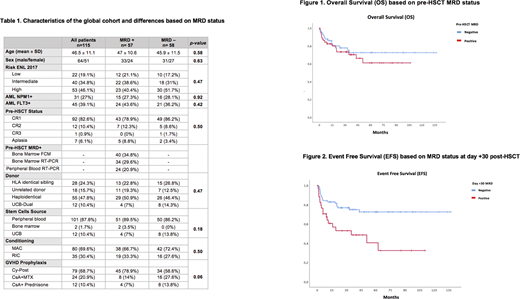
A total of 115 patients were analyzed. Pre-HSCT MRD was negative in 58 patients (50.4%) and positive in 57 patients (49.6%). We found no statistically significant differences in the characteristics between the two groups (Table 1).
Median follow up was 39 months (IQR 10.4-55.8). 3-year overall survival (OS) for patients with pre-HSCT negative MRD was 72.5% versus 70.3% in patients with positive MRD (p=0.41), with an event free survival (EFS) of 66.9% versus 66.1 (p=0.48) respectively (Figure 1).
Median time to the beginning of immunosuppression withdrawal was 82.5 days (IQR 59-93) for patients with negative MRD and 68 days (IQR 55.3-85.3) for patients with positive MRD (p<0.001). The cumulative incidence of grade II-IV acute graft versus host disease (aGVHD) and moderate-severe chronic GVHD did not show statistically significant differences based on the MRD status. Similarly, the cumulative incidence of relapse and the 2-year mortality was not significantly different between the two groups.
Patients with negative MRD at day +30 showed a 2-year OS of 83.5% versus 58.1% in patients with positive MRD (p=0.03) and a EFS of 79.9% versus 48.6% (Figure 2). The cumulative incidence of relapse was more elevated in patients with positive MRD (29.8% versus 13.6%) at day +30.
Patients with mixed chimerism (MC) at day +30 showed a significantly lower 3-year OS and EFS than patients with complete chimerism (CC). Likewise, the cumulative incidence of relapse was significantly higher in patients with MC, both if detected in bone marrow aspirate and in CD34+ cells.
The multivariate analysis revealed that MRD status at day +30 post-HSCT was an independent prognostic factor for EFS (HR 3.74; 95% CI 1.38-10.1; p=0.009).
CONCLUSIONS
Patients with AML presenting a positive MRD in the early post-HSCT period and those who show a MC at day +30 post-HSCT have lower EFS, with positive MRD at day +30 being an independent prognostic factor for EFS. The evaluation of MRD and chimerism in the early post-HSCT period is useful to identify patients with higher risk of relapse, who may take advantage of preemptive measures.
Kwon:Gilead, Novartis, Pfizer, Jazz: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal