

ABSTRACT
Introduction:Patients with indolent non-Hodgkin lymphomas (iNHL), including follicular lymphoma (FL), have high response to first-line treatment. However, retreatment is often required when relapses occur, and those with multiple relapses represent a patient population with an unmet need for effective treatment. Clinical data for several treatment options exist for the general relapsed and refractory (R/R) population; however, there are relatively fewer data specific to FL patients with ≥2 lines of prior treatment. This work systematically identified the available efficacy data in the double R/R FL population.
Methods:The MEDLINE and EMBASE databases were searched through February 10, 2020. Studies were limited to interventional clinical trials of R/R FL patients (or mixed histologies with a predominance of FL) and articles published in English. Studies also must have reported one or more efficacy measures, such as overall response rate (ORR), complete response (CR), duration of response (DoR), time to next treatment (TTNT), progression-free survival (PFS), and overall survival (OS). Potential interventions of interest were lenalidomide ± rituximab (R), duvelisib, ibrutinib, venetoclax, polatuzumab vedotin + R, obinutuzumab, copanlisib, umbralisib, idelalisib, and tazemetostat.
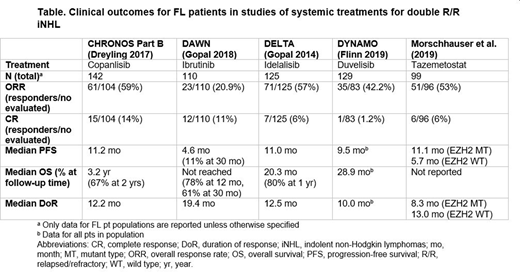
Results:Of 35 publications examining treatment outcomes in R/R FL patients, only 14 (representing 5 unique clinical trials) were specific to the ≥ 2-line population. These trials were: CHRONOS Part B (copanlisib), DAWN (ibrutinib), DELTA (idelalisib), DYNAMO (duvelisib), and Morschhauser et al. 2019 (tazemetostat) and included a total of 605 participants. All studies used similar inclusion criteria, and patients included were similar in age (median 62-65), disease stage (III/IV), and ECOG score (0-2). Patients in the CHRONOS study had a median number of prior treatments of 2, whereas those in the DELTA study had 5. ORR ranged from 21% (ibrutinib) to 59% (copanlisib) (Table). The DoR ranged from 8.3 months in tazemetostat patients with EZH2 gene mutation to 19.4 months for ibrutinib. PFS ranged from 5.7 months in tazemetostat patients with wild-type EZH2 to 11.2 months for copanlisib. Median TTNT was only reported in the DAWN study (16 months).
Conclusions:Very few clinical data exist reporting efficacy outcomes specific to the double R/R FL population. The limited data indicate that current treatments do not produce durable responses for most double R/R FL patients, demonstrating an unmet need. Further research is needed to fully understand the efficacy and safety of other potential interventions for this population.
Kahl:Genentech:Consultancy;Pharmacyclics LLC:Consultancy;AstraZeneca Pharmaceuticals LP:Consultancy, Membership on an entity's Board of Directors or advisory committees;ADC Therapeutics:Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding;Celgene Corporation:Consultancy;AbbVie:Consultancy;Roche Laboratories Inc:Consultancy;BeiGene:Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding;Janssen:Consultancy, Membership on an entity's Board of Directors or advisory committees;Acerta:Consultancy, Research Funding.Patel:Kite, a Gilead Company:Current Employment.Zaidi:BMS:Consultancy.Snedecor:Pharmerit - an OPEN Health Company:Other: Employment at consultancy paid by Kite Pharma to conduct this work.Purdum:Kite, a Gilead Company:Current Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal