

Introduction:
Hemorrhagic cystitis (HC) due to viral infections, such as BK virus, cytomegalovirus and/or adenovirus, after Allogeneic Hematopoietic Cell Transplantation (allo-HCT) causes morbidity and mortality, impacts quality of life, and poses a substantial burden to the health care system. Virus-associated HC (V-HC) occurs in up to 25% and 54% of pediatric and adult allo-HCT recipients respectively. V-HC is associated with incapacitating pain, life-disturbing urinary symptoms, and in severe forms, severe hematuria requiring transfusion support, bladder obstruction, renal impairment and increased mortality. At present, management is purely supportive as there are no approved or recommended anti-virals for V-HC. The impact of V-HC on health resource utilization (HRU) and HCT outcomes has not been studied at a national level. The objective of this study was to compare the economic burden, HRU and clinical outcomes among allo-HCT recipients with V-HC to those without V-HC using a large US claims database.
Methods:
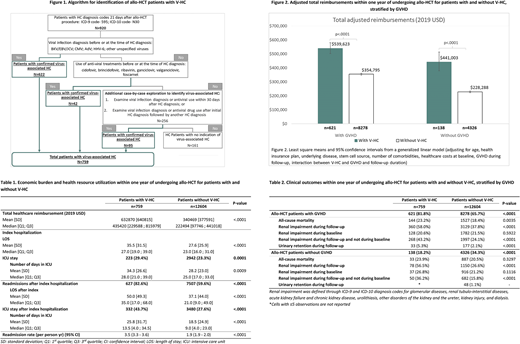
A US claims database obtained from the Decision Resources Group Real World Evidence Data Repository was used to identify patients with first (index) allo-HCT procedure from 1/1/2012-12/31/2017. The 1-year period prior to the index allo-HCT was considered as the baseline period. Although, there are diagnosis codes in the International Classification of Diseases (ICD-9 or ICD-10) coding system for HC, there are no specific diagnosis codes to identify V-HC. Hence, an algorithm was developed through clinical guidance to identify these patients among those with HC diagnosis codes (Figure 1).
Outcomes were examined in the 1-year post allo-HCT and included total healthcare reimbursements, HRU and clinical outcomes for allo-HCT patients with vs. without V-HC. Total reimbursements were estimated from submitted charges using a reimbursement-to-charge ratio of 0.425 and were reported in 2019 US dollars, adjusted using the medical care component of the US Consumer Price Index. Further, a generalized linear model was used to determine adjusted reimbursements stratified by the presence or absence of any acute or chronic graft-versus-host diseases (GVHD) after adjusting for age, health plan, underlying disease, stem cell source, number of comorbidities, baseline costs, and follow-up time.
Results:
Of 13,363 allo-HCT recipients, 759 (5.7%) patients met the criteria for V-HC. Total unadjusted mean reimbursement was $632,870 (SD=$640,815) for patients with V-HC and $340,469 (SD=$377,591) for patients without V-HC (Table 1). In multivariable model after adjusting for confounders, the adjusted reimbursements were significantly higher for V-HC patients with and without GVHD compared to patients without V-HC (p<.0001) (Figure 2).
V-HC was associated with increased hospital length of stay (LOS) and readmission rates. Patients with V-HC had 7.9 additional days in the hospital (35.5 vs 27.6 days; p<.0001) and 6.1 additional days (34.3 vs. 28.2 days; p=0.0009) in the intensive care unit (ICU) for the index hospitalization, as compared to patients without V-HC (Table 1). The hospital readmission rate was higher for allo-HCT patients with V-HC compared to those without V-HC (3.5 vs. 1.9 per person yr; p<.0001), resulting in 12.9 more days in the hospital (50.0 days vs. 37.1 days; p<.0001) and 7.3 more days in the ICU (25.8 days vs. 18.5 days; p<.0001) after the index hospitalization (Table 1).
V-HC was associated with increased mortality in patients with GVHD and increased risk of renal impairment in all allo-HCT patients. Among patients with GVHD, those with V-HC had significantly higher all-cause mortality as compared to those without V-HC (23.2% vs. 18.4%; p=0.0035) (Table 2). When stratified by GVHD, there were no significant differences in the baseline risk for renal impairment; while V-HC was associated with increased risk for renal impairment in the follow-up period in patients with or without GVHD (p<.0001 for both) (Table 2).
Conclusions:
Allo-HCT patients with V-HC have significantly higher healthcare reimbursements, health resource utilization, and worse clinical outcomes including renal impairment, irrespective of the presence of GVHD; with significantly higher all-cause mortality in the presence of GVHD. Our results highlight the unmet clinical need for effective strategies to prevent and treat V-HC in HCT recipients that may also reduce costs among these patients.
McGuirk:Pluristem Ltd: Research Funding; Juno Therapeutics: Consultancy, Honoraria, Research Funding; Astellas: Research Funding; Kite Pharmaceuticals: Consultancy, Honoraria, Research Funding, Speakers Bureau; Fresenius Biotech: Research Funding; Novartis: Research Funding; Gamida Cell: Research Funding; Bellicum Pharmaceutical: Research Funding; Allo Vir: Consultancy, Honoraria, Research Funding. Moon:AlloVir, Inc.: Current Employment, Current equity holder in publicly-traded company. Chandak:AlloVir, Inc.: Other: Independent contractor. Zhang:AlloVir, Inc.: Other: Independent contractor. Papanicolaou:Chimerix: Other: Consulting and other fees, Research Funding; Astellas Pharma: Other: Consulting and other fees, Research Funding; Merck & Co.: Other: Consulting and other fees, Research Funding; Octapharma: Other: Consulting and other fees; Partner Therapeutics: Other: Consulting and other fees; ADMA Biologics: Other: Consulting and other fees; Shionogi: Other: Consulting and other fees; Cidara: Other: Consulting and other fees; Amplyx: Other: Consulting and other fees; Siemens: Other; Takeda: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal