

Introduction
The outcomes related to different anticoagulation doses in Coronavirus disease 2019 (COVID-19) patients are not well established. COVID-19 is associated with increased thrombotic events and early coagulopathy as reported by a large New York City health system.
Initial studies on patients in Wuhan, China showed anticoagulant therapy mainly with low molecular weight heparin was reported to be associated with better prognosis in severe COVID‐19 patients meeting sepsis‐induced coagulopathy criteria or with markedly elevated D‐dimer. These studies fueled the need for anticoagulation protocols to be institutionalized broadly.
Here we report the outcomes of patients on prophylactic compared to treatment dose anticoagulation early in the COVID-19 pandemic. This data reflects results before broad institutionalization of anticoagulation protocols for this novel disease in a Brooklyn, New York population.
Methods
This is a retrospective chart review of all laboratory confirmed COVID-19 patients who were admitted to New York-Presbyterian Brooklyn Methodist Hospital between March and April, 2020. Patient clinical characteristics were manually extracted from electronic medical records. Patients were divided into 2 groups: patients on treatment dose anticoagulation and patients on prophylactic dose anticoagulation. Primary outcome of this study was inpatient mortality among the two groups. Secondary outcomes were thromboembolisms (both arterial and venous), myocardial infarction (MI), major bleeding, ICU admission, ICU length of stay, invasive mechanical ventilation and initiation of dialysis. Odds ratio and p-values were obtained using univariate analysis.
Results
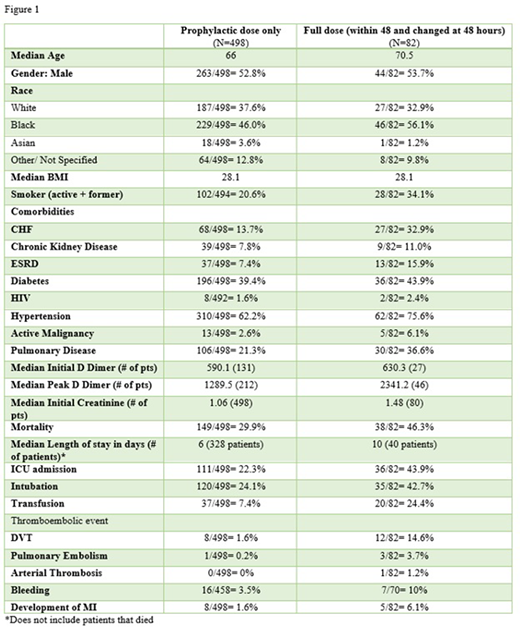
We analyzed 580 hospitalized patients with confirmed nasopharyngeal COVID19 infection. Of these, 82 patients were on treatment dose anticoagulation 498 patients were on prophylactic dose. Median age was 70 years in treatment dose group and 66 years in prophylactic dose group. Percentage of males were similar between both groups (53%). African American race(56% vs 46%) was the predominant race in both groups. Median BMI was 28.1 in both groups. Percentage of smokers was higher in the treatment dose group (34% compared to 21%). Patients in the treatment dose group had a higher rate of all the comorbidities. Median D-Dimer (630 vs 590) was higher in the treatment dose group.
Rates of ICU admission in treatment dose group and prophylactic dose group was 44% and 22% respectively. Patients requiring intubation (43% vs 24%) and transfusion (24% and 7%) were higher in the treatment dose group. There was an increased incidence of thromboembolic events in the treatment dose group as compared to prophylactic dose group with DVT (15.6% vs 1.6%) PE (3.7% vs 0.2%), arterial thrombosis (1.2% vs 0%) and MI (6.1% vs 1.6%). Incidence of major bleeding was higher in the treatment group (10% vs3.5%)
Discussion
Our study found increased inpatient mortality with treatment dose anticoagulation and increased risk of bleeding when compared with prophylactic dose anticoagulation. These findings may be due to higher rates of comorbidities, smoking and older age when compared to the prophylactic anticoagulation group. Higher rates of bleeding raises concern for the safety of treatment dose anticoagulation in these populations.
Some limitations of this study include: uneven sample size between the two groups and data was collected from patients before anticoagulation dose recommendations were standardized and officially implemented. Further randomized control trials are needed to evaluate the dose- dependent relationship between anticoagulation and mortality.
Our study suggests that the treatment dose anticoagulation may adversely affect the outcomes in COVID-19 patients who are older and have multiple comorbidities. Therefore, the anticoagulation dose must be chosen carefully given the overall clinical picture.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal