

Background
Multiple myeloma (MM) is a hematologic malignancy resulting from clonal proliferation of plasma cells in the bone marrow (BM). The BM tumor microenvironment confers therapeutic resistance through survival and growth signals to myeloma cells and suppression of anti-tumor immune responses. A population of myeloid-derived suppressor cells (MDSCs), abundantly producing the pro-inflammatory S100A9 protein, promotes myeloma progression. Tasquinimod (TASQ) is an investigational drug that targets MDSCs via the S100A9 protein. In pre-clinical models of MM, TASQ has significant anti-tumor effects as a single agent and in combination with bortezomib, a proteasome inhibitor (PI) and lenalidomide, an immunomodulator (IMiD) (Lin C, et al. 25th Annual Meeting of European Hematology Association June 11-21 2020: EP896). TASQ has previously been studied as a novel, once-daily oral anti-cancer agent, including in a phase-3 randomized trial in patients (pts) with metastatic prostate cancer that showed improvement in radiographic progression-free survival (Sternberg C, et al. JCO 2016; 34(22): 2636-43). The side effect profile of TASQ is well-characterized based on this previous experience.
We therefore designed a phase 1 trial (NCT04405167) to establish the maximum tolerated dose (MTD) and optimal schedule for TASQ in MM and then investigate the MTD of TASQ in combination with a standard oral myeloma regimen of ixazomib, lenalidomide, and dexamethasone (IRd). For both single agent TASQ and the combination of TASQ with IRd, exploratory expansion cohorts will be enrolled to preliminarily characterize the antimyeloma activity of each regimen.
Study Design
Enrolled pts must have MM relapsed or refractory after at least one prior line of anti-MM therapy. Other key inclusion criteria include measurable disease and Eastern Cooperative Oncology Group performance status ≤2. Key exclusion criteria include failure to have fully recovered from clinically significant adverse effects of prior chemotherapy; active graft versus host disease; treatment with cytotoxic chemotherapy within 3 weeks prior to initiation of study treatment; treatment with PIs, IMiDs, or monoclonal antibodies within 2 wks, experimental therapy or plasmapheresis within 4 wks, or systemic corticosteroids or radiotherapy within 7 days; known central nervous system involvement by myeloma; or a diagnosis of smoldering MM or POEMS syndrome, active plasma cell leukemia, symptomatic primary amyloidosis, or myelodysplastic or myeloproliferative syndrome.
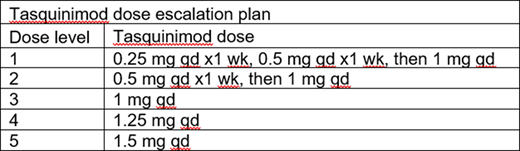
Single agent TASQ and the combination of TASQ with IRd will be investigated in two parts. Part A will start with dose-escalation of single agent TASQ using a standard 3+3 design, with 3 to 6 pts evaluable for dose-limiting toxicity at each dose-level (see table). In the subsequent expansion cohort, additional pts will enroll at the MTD/optimal schedule, so that 12 pts total evaluable for response will have received the MTD/optimal schedule of single agent TASQ. Part B combines TASQ with standard-dose IRd: 28-day cycles of ixazomib 4 mg on days 1, 8, and 15, lenalidomide 25 mg on days 1-21, and dexamethasone 40 mg on days 1, 8, 15, and 22. The part B dose-escalation starts at the lower of either dose-level 1 or one dose-level below the single agent MTD. Additional pts with disease refractory to their most recent PI/IMiD combination will enroll into a part B expansion cohort, so that 12 pts total who are both evaluable for response and PI/IMiD refractory will have received the MTD/optimal schedule of TASQ in combination with IRd. Treatment will continue until unacceptable toxicity or myeloma progression.
The primary study endpoint is the MTD of TASQ as single agent and in combination with IRd. Key secondary endpoints include toxicity (treatment-emergent grade 3/4 adverse events using the National Cancer Institute Common Toxicity Criteria for Adverse Events, version 5), preliminary antimyeloma activity (using the response criteria of the International Myeloma Working Group), changes in the BM microenvironment, and systemic TASQ exposure during therapy with single-agent TASQ and during therapy with TASQ in combination with IRd. These results will determine whether TASQ, alone or combined with standard anti-MM therapy, represents a promising novel treatment strategy in MM.
Vogl:Active Biotech: Consultancy, Research Funding; Janssen: Consultancy; Karyopharm: Consultancy; Takeda: Consultancy; Celgene: Consultancy; Oncopeptides: Consultancy; MorphoSys: Consultancy. Nefedova:Active Biotech: Consultancy, Research Funding. Bondesson:Active Biotech: Current Employment. Eriksson:Active Biotech: Current Employment. Tuvesson:Active Biotech: Current Employment.
Tasquinimod for multiple myeloma

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal