

Introduction:
Imaging of brain oxygenation can be a powerful tool to assess the risk of stroke in patients with sickle cell disease (SCD), and may potentially aid in stroke prevention. Currently, there is disagreement in oxygen extraction fraction estimated by techniques that measure tissue oxygenation from deep brain structures, and techniques that measure blood oxygenation in the sagittal sinus. Quantitative susceptibility mapping (QSM) is an MRI technique that can noninvasively measure venous blood oxygen saturation (SvO2) in deep cerebral structures based on the magnetic susceptibility shift of venous blood caused by deoxyhemoglobin. In this study, our goal was to compare venous oxygen saturation measured by QSM in the internal cerebral vein (ICV) to venous oxygenation in the sagittal sinus (SS) in SCD patients, anemia subjects with normal hemoglobin and healthy controls.
Methods:
16 SCD patients, 7 non-sickle anemia patients and 11 healthy controls participated in the study(Table 1). All subjects provided written consent to a protocol approved by the Committee on Clinical Investigation (CCI#11-00083).
Images were acquired on a clinical 3 T Philips system with a 32-channel RF coil. The 3D gradient echo sequence had parameters: TR = 30 ms, α = 25°, 2 echoes: TE1 = 4.94 ms, ΔTE = 5.2 ms, FOV = 210 x 190 x 120 mm, spatial resolution: 0.6 x 0.6 x 1.3 mm, SENSE acceleration rate = 2 in the phase-encoding direction, BW = 289 Hz/pix and total acquisition time = 6 mins 50 seconds. Flow-compensation was added in the readout direction only, which was the anterior-posterior (AP) direction.
For each subject, phase images were fitted to generate a B0 field map. Brain extraction and phase unwrapping was performed using FSL. Background field was removed using PDF. Unreliable phase voxels were identified and removed from the brain mask for subsequent processing. L1-regularized field-to-susceptibility inversion was performed to derive the susceptibility map (lambda = 4*10-4). Venous oxygen saturation was computed based on:
χ = (1 - SvO2)χd-oHct + χo-wHct [1]
where χ is the susceptibility measurement of the ICV, χd-o is the susceptibility shift per unit hematocrit between fully oxygenated and fully deoxygenated erythrocytes, and χo-w is the susceptibility shift between oxygenated blood cells and water. Values of 0.27 ppm (c.g.s unit) and -0.03 ppm were used for χd-o and χo-w.
The ROI mask of the ICV was manually selected based on the susceptibility map that was threshold at 0.1 ppm to avoid partial-volume effect. Only the segment that had an angle below 30 degree with respect to the AP axis was included. The purpose was to exclude regions that were susceptible to flow artifact. Intra-ROI average venous oxygen saturation were computed. Group difference of venous oxygen saturation was tested using Student t-test.
Results:
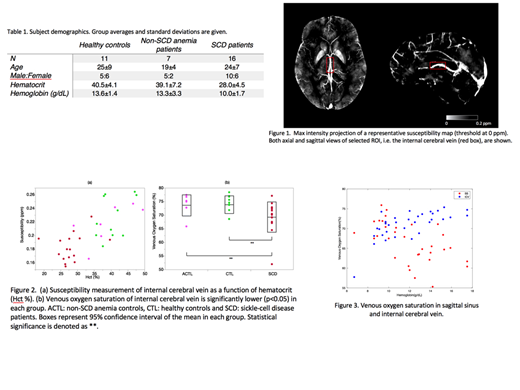
Figure 2a shows ICV magnetic susceptibility increases linearly with hematocrit as predicted by Eq [1]. Mean ICV venous oxygen saturation in the three groups was 73.9% in CTL, 73.6% in ACTL, compared with SCD 69.3%, p<0.05 by analysis of variance. Figure 3 compares the ICV and SS oxygen saturation as a function of hemoglobin concentration. At normal hemoglobin values, SS saturation was lower than in the ICV, but this difference disappeared with increasing anemia severity. After controlling for hemoglobin value, there were no patient group differences in oxygen saturation in either location.
Discussion:
In non-anemic subjects, SS oxygen saturation was lower than in the ICV, potentially reflecting increased oxygen demand of the cerebral cortex compared with deep brain structures. ICV is one of the major deep cortical veins, and oxygen saturation of this vein can indicate the oxygenation of deep structures of the cerebral hemispheres, including the basal ganglia, corpus callosum and thalamus. With progressive anemia, brain blood flow increases to preserve cerebral oxygen delivery (not shown), but favors grey matter perfusion at the expense of deep white matter structures. This could explain the decline in venous saturation with hemoglobin seen in the ICV compared with the rise in venous saturation observed in the SS. Alternatively, global increases in flow may homogenize and shorten microvascular transit times, equalizing the oxygen extraction across brain vascular territories.
Coates:celgene: Consultancy, Honoraria, Other: steering committee of clinical study; agios pharma: Consultancy, Honoraria; vifor: Consultancy, Honoraria; apo pharma: Consultancy, Honoraria, Speakers Bureau. Wood:Apopharma: Consultancy; BiomedInformatics: Consultancy; National Institutes of Health: Research Funding; Imago Biosciences: Consultancy; WorldcareClinical: Consultancy; Philips Healthcare: Research Funding; BluebirdBio: Consultancy; Celgene: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal