

Background: Sperm parameters alteration is documented in untreated men with sickle cell disease (SCD). An aggravating effect of hydroxyurea (HU) on sperm parameters is also well established: HU, at current doses, causes significant, rapid, and unpredictable impairment of spermatogenesis. Reversal of its effect when treatment is stopped has also been documented, albeit in patients given very low doses of treatment (10 mg/kg/d). In France, sperm banking is free of charge and recommended whenever possible before initiation of HU treatment. While recent guidelines have broadened the indication of HU for asymptomatic infantssuch banking is impossible in younger boys before puberty. In addition, little is known on the effect of HU on sperm parameters when given at this specific period.
Objectives and Methods: The main objective of this study was to compare sperm parameters after treatment resolution in young males treated by HU prior to puberty with sperm parameters of untreated males. Secondary objective was to analyze longitudinally sperm parameters during HU washout in those treated prior to puberty.Data regarding indication of HU, dosage, date of initiation and stop, clinical profile including vaso occlusive events (VOE) transfusion episodes and date of puberty was collected. Alternative treatment before or during semen analysis was also documented. A period of 3 months of HU wash out was required prior to semen analysis in treated patients.
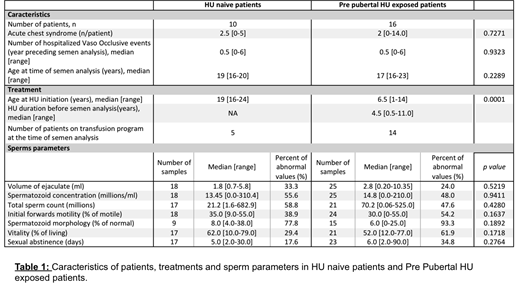
Results: A total of 26 patients (43 semen samples) were studied, with 16 patients treated with HU prior to puberty (HU-PP) and 10 untreated (HU-naive). Characteristics of patients are presented in Table 1. Indication of HU was cerebral vasculopathy (n=3), VOE (n=5), severe anemia (n=1) or combined (n= 7). The median stopping of the HU before CECOS is 4.5 years [0.5-11.0]. An alternative treatment based on a transfusion program was initiated in 14 patients (87.5%) at the time of sperm analysis in the HU-PP group versus 5 patients (50%) in the HU-naive group. Duration of transfusion program was 126 months [3-188] in HU-PP versus 13 [7-100] in the HU naive group.
We compared the fraction of abnormal values in semen samples in both groups (25 samples in the HU-PP group and 18 in the HU-naive). No significant difference was observed regarding volume of ejaculate, spermatozoid concentration, total sperm count, spermatozoid motility, morphology and vitality, and sexual abstinence before sampling in both groups (Table 1). In the HU-PP group, there was a trend in improvement of sperm parameters with the duration of transfusion program. In addition, a kinetic analysis of sperm parameters during the period of HU wash out was performed in 3 patients exposed to HU prior to puberty, demonstrating reversibility of HU toxicity in all.
All 26 patients were offered semen cryopreservation. For 22 of them, semen parameters after thawing indicated a possible use for assisted reproductive technologies, mostly in vitro fertilization with intracytoplasmic sperm injection. In the remaining 4 (3 in HU-PP group and 1 in HU naïve), there was serious concern about the possible use because of a very low initial sperm concentration and the absence of motile spermatozoids after thawing.
Discussion/Conclusion: Toxicity of HU upon spermatogenesis has been well documented in animal studies and in adult males. In many settings, such issues may be a drawback for parents and/or caregivers to treat young boys before semen banking can be performed, given the lack of robust information on reversibility after treatment resolution. Abnormalities of sperm count are also common in non-treated males so that demonstrating the specific effect of HU may be complex. Oseggbe et al. and Berthaud et al. showed that 91% of untreated SCD males have at least one abnormal sperm parameter. Here, we show that after treatment resolution, there are no differences in sperm parameters in patients exposed to HU before puberty compared to untreated males. Because a majority of patients benefitted from transfusion therapy at the time of analysis, we were however unable to demonstrate whether reversal of toxicity occurs spontaneously or requires transfusion. Notwithstanding possible limitations due to small sample size, this study shows that in boys with severe disease requiring HU treatment before puberty, toxicity of HU on sperm parameters should not be a major drawback.
Bernaudin:AddMedica: Honoraria, Other: Help for travel; GBT: Membership on an entity's Board of Directors or advisory committees; BlueBirdBio: Consultancy. De Montalembert:Novartis: Consultancy, Honoraria; Addmedica: Consultancy, Honoraria; Bluebird Bio: Membership on an entity's Board of Directors or advisory committees. Brousse:bluebird bio: Consultancy; Add medica: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal