

Background: TBdepl-haploHSCT is a suitable option for children with AL in need of an allograft, lacking an HLA-compatible donor. We previously published promising results in a cohort of 80 children with AL, given this type of allograft (Locatelli et al., Blood 2017), demonstrating a low incidence of acute and chronic graft-versus-host disease (GvHD) and low non-relapse mortality (NRM), translating into a final outcome comparable to that of patients transplanted from an HLA-compatible donor. We present the long-term follow-up analysis of this study (NCT01810120), now including 134 patients, with a minimum observation time of 100 days after the allograft.
Patients and methods: Between October 2010 and April 2019, 134 children with AL in morphological complete remission (CR) received TBdepl-haploHSCT from an HLA-partially matched relative (a parent in 97% of cases) at Ospedale Pediatrico Bambino Gesù in Rome, Italy. All patients were prepared to the allograft using a fully-myeloablative conditioning regimen including a combination of cytotoxic drugs and/or total body irradiation (TBI). Anti-T-lymphocyte globulin (ATLG) was used before transplantation (12 mg/kg total dose, from days -5 to day -3) to modulate bi-directional donor/recipient alloreactivity. Rituximab (200 mg/sqm) was administered on day -1 to prevent post-transplantation EBV-induced lymphoproliferative disorders (PTLD). No patient received any post-transplant GvHD prophylaxis.
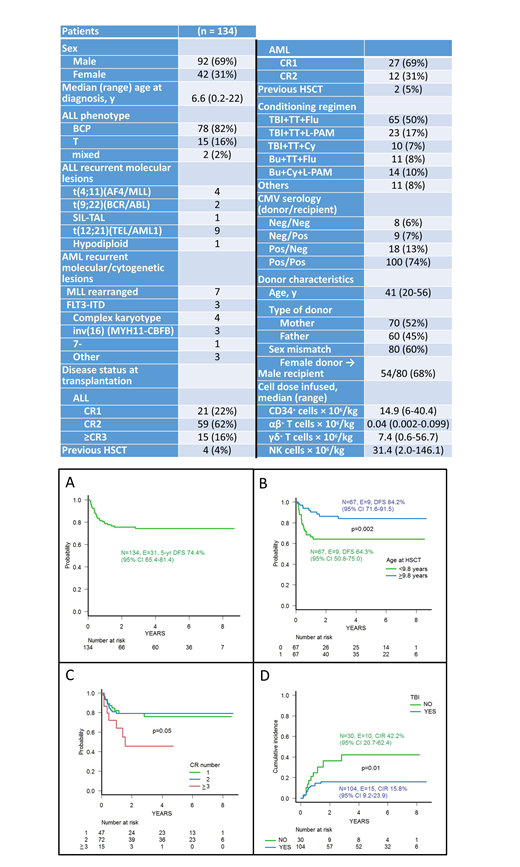
Results: Characteristics of patients enrolled in the study are shown in Table 1. Median follow-up of surviving patients is 60 months (range: 3 months - 8.7 years). Only 3 patients did not achieve engraftment (all affected by acute myeloid leukemia and who did not receive TBI during conditioning regimen); median time to neutrophil and platelet recovery was 13 (range 9-22) and 11 (range 8-23) days, respectively. Cumulative incidence of grade II-III acute GvHD was 16.5% (95% CI 9.9-22.6). One patient developed gut GvHD, while for all other patients skin was the sole organ involved; no case of grade IV GvHD was recorded. Eight out of the 123 patients at risk developed chronic GvHD, in all cases of limited severity, the cumulative incidence of this complication being 7.6% (95% CI 2.3-12.6). Six patients died for transplant-related complications (2 because of idiopathic pneumonitis and 1 each of disseminated adenovirus infection, cardiac insufficiency, combined CMV/rhinovirus pneumonia and sepsis from Pseudomonas aeruginosa), the 5-year cumulative incidence of NRM being 4.5% (95% CI, 1.8-9.0). Since 25 patients relapsed at a median time of 173 days (range 59-1012) after HSCT, the 5-year cumulative incidence of relapse is 21.1% (95% CI, 14.2-29.1). The 5-year probability of overall and leukemia-free survival (LFS) were 74.6 (95% CI 65.1 -71.9) and 74.4% (95% CI 65.4-81.4) (Figure 1A), respectively. Use of TBI during the preparative regimen, age at transplant above the median value (Figure 1B) and disease status at transplantation (CR1 and CR2, Figure 1C) were associated with better patient's outcome, because of a reduced incidence of relapse (Figure 1D for TBI). All these 3 factors remained statistically significant in multivariable analysis for LFS: hazard ratio (HR) for TBI was 0.16 (95% CI, 0.06- 0.37, p<0.001, HR for age at HSCT was 0.27 (95% CI, 0.11-0.65, p=0.003), while that for disease status was 0.49 (95% CI, 0.26-0.91, p=0.02), respectively. The 5-year GvHD/relapse-free survival was 69.9% (95% CI 60.8-77.3). The median CD3+ cell count on day +30, +90, +180 and +360 were 187, 215, 660 and 1260/mcl, respectively.
Conclusions: These data confirm in a larger population and with a longer follow-up that TBdepl-haploHSCT is a safe and effective transplant option, being associated with a low risk of both NRM and acute/chronic GvHD, resulting into a 5-year LFS comparable or even better with that reported in studies using either an HLA-identical sibling or an unrelated volunteer as donor. In particular, the low incidence of chronic GvHD preserves a good quality of life in patients with long life-expectancy. Leukemia recurrence represents the main cause of treatment failure and strategies based either on the use of a titrated number of donor T cells transduced with a safety switch or ex-vivo depleted of the alloreactive component could further improve patient's outcome.
Merli:Novartis: Honoraria; Sobi: Consultancy; Amgen: Honoraria; Bellicum: Consultancy. Algeri:Miltenyi: Honoraria; Atara Biotherapeutics: Consultancy, Honoraria; Bluebird bio: Consultancy, Honoraria. Locatelli:Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Bellicum: Consultancy, Membership on an entity's Board of Directors or advisory committees; bluebird bio: Consultancy; Miltenyi: Honoraria; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal