

Background: Survival of patients with MM has improved significantly over recent years due to therapeutic advancements. Population-level data has shown that a substantial proportion of MM patients may die early after their diagnosis and real-world evidence regarding early mortality (≤6 months after MM diagnosis) has been conflicting. We evaluated the trends, causes and predictors of early mortality among newly diagnosed MM (NDMM) patients in the real world.
Methods: We used Surveillance Epidemiology and End Results (SEER) database, to identify all adult patients (age ≥ 18 years) who were diagnosed of MM from 1975 to 2015. Data on age, gender, geographical regions, year of diagnosis, survival time, vital status at 6 months after diagnosis and cause of death (COD) were extracted. Ages were categorized as quartiles while period of diagnosis for multivariate analysis were categorized by running a joinpoint analysis separately for the all-cause and myeloma-specific mortality. To look at trends in early mortality, we estimated proportion of deaths for each year and plotted it as a scatterplot against the year of diagnosis and fitted it in the join point regression model by applying the NCI's Join point Regression Program, Version 4.5.0.1. By this method we identified the year(s) when a trend change was produced, calculated the annual percentage change (APC) in rates between trend-change points, and the average annual percentage change (AAPC) in the whole period studied. To correct for known errors with COD attribution, we applied a special COD variable which has been recently developed by the SEER program to indicate if the death was due to the primary cancer diagnosis or other causes. A multivariate analysis was conducted to analyze the predictors of all-cause and myeloma-specific mortality within 6 months by fitting into logistic regression model.
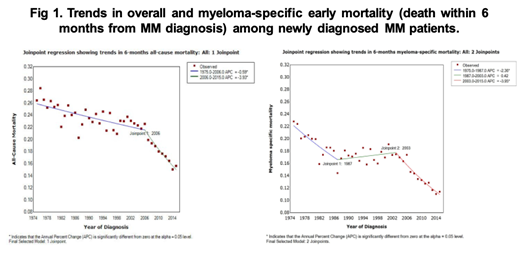
Results: Of 90,975 NDMM patients, early mortality due to any cause was noted in 18,810 (20.7%). For the whole cohort, median age was 68 years, majority of the patients were males (53.1%), of non-Hispanic white (NHW) race/ethnicity (65.5%) and were diagnosed in SEER registries in the western region (53.9%). An overall survival (OS) of ≤6 months was seen for approximately 22% of NHW but 18% of non-Hispanic blacks (NHB) and Hispanics. OS of ≤6 months was seen in 10% of patients in the first quartile of age (<60 years) as compared to 36% of patients in the 4th quartile (≥78 years). By geographical regions, 23.3% of MM patients in the Midwest had ≤6-month OS as compared to only 18.4% in the Northeast. The most common early mortality COD was MM in 74.7% of the patients, followed by cardiovascular (11.9%), other (8.8%) and infectious causes (3.1%). The overall pattern of COD at 6 months was similar to COD at any time in the whole cohort. Joinpoint regression analysis of trends data resulted in 1 joinpoint for all-cause 6-month mortality while 2 joinpoints were noticed for myeloma-specific mortality (Figure 1). A steep decline in mortality was noticed in the more recent time periods for both, all-cause (2006-2015) and myeloma-specific (2003-2015) mortality rates with an AAPC of 3.93 (95%CI p<0.001) for all-cause and 3.95 (95%CI p<0.001) for myeloma-specific mortality. Prior to 2006, the decrease in all-cause mortality was only modest whereas decrease in myeloma-specific mortality witnessed a sharp decline from 1975-1987 as well. On MVA, advanced age (p<0.001), NHW race/ethnicity and Midwest geographic region (p<0.001) were associated with higher likelihood of mortality while female gender (p<0.001), more recent period of diagnosis (p<0.001), and "other" races (not NHW, NHB or Hispanics) (p<0.001) were associated with lower risk of mortality.
Conclusion: Our results show that early mortality due to MM remains high despite therapeutic improvements and there are significant gender, racial and geographic disparities for this phenomenon. However, significant declines in all-cause and MM-specific early mortality in the more recent times are promising. The risk of early mortality is higher among men, older patients, NHW and Midwest region. A focus on interventions to reduce early mortality, including early diagnosis, use of efficacious anti-MM therapy and aggressive supportive care should be directed at groups with high-risk for early mortality from MM.
Chanan-Khan:Millennium: Research Funding; Ascentage: Research Funding; AbbVie: Research Funding; Xencor: Research Funding; Pharmacyclics: Research Funding; Merck: Research Funding; Jansen: Research Funding; Mayo Clinic: Employment. Ailawadhi:Celgene: Consultancy; Pharmacyclics: Research Funding; Amgen: Consultancy, Research Funding; Takeda: Consultancy; Cellectar: Research Funding; Janssen: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal