

Introduction
Per the National Cancer Institute epidemiological data, the incidence of multiple myeloma has not changed significantly over the past decade. Mortality from myeloma has not changed significantly between 2007-2016 with an estimated 5-year survival of 55.2 % between 2009-2015. The treatment of multiple myeloma has improved significantly over the past decade with the approval of several new drugs. In the recent IFM trial, the 4-year overall survival in a select group of myeloma patients was 82% when treated with bortezomib, lenalidomide and dexamethasone followed by autologous stem cell transplant and maintenance therapy. These numbers may further improve with approval of monoclonal antibodies and several new drugs in clinical trials.
The cost of healthcare has been growing consistently for the past several years. Per CMS data, healthcare spending grew 3.7% in 2017 reaching $3.5 trillion, or $10,739 per person. National health spending is projected to grow at a rate of 5.5% per year from 2018-2027 reaching nearly $6.0 trillion. Health share of the GDP is expected to rise from 17.9% to 19.4%. Pharmaceutical costs have been rising consistently over the past several years with cancer therapies being some of the costliest. Most new cancer therapy costs more than $100,000 per year with the triplet combinations for myeloma costing upwards of $200,000 per year.
Methods
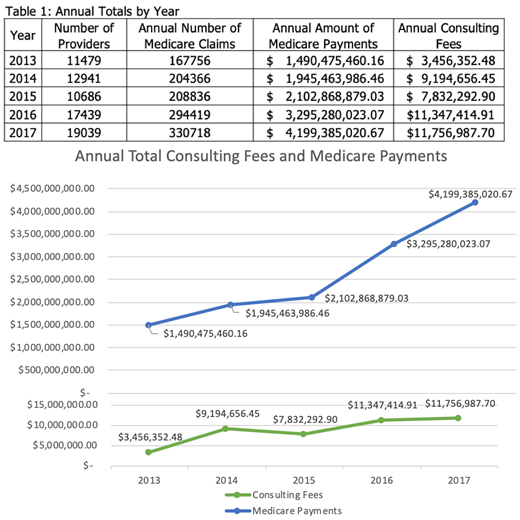
Our goal was to evaluate the utilization of the newer drugs approved for myeloma by the Medicare population and assess the economic burden of growing drug prices on the health care system. We queried the national CMS database from 2013-2017 to obtain information on Medicare payments made, number of providers making claims and consulting fees for bortezomib, carfilzomib, daratumumab, elotuzumab, ixazomib, lenalidomide, panobinostat and pomalidomide.
Results
Between 2013-2017 there has been a significant increase in the annual Medicare payments made for myeloma drugs. The amount of payments has tripled between 2013-2017. The number of claims made and providers making those claims have increased. There has also been an exponential increase in consulting fees paid by various pharmaceutical companies to promote prescription of the aforementioned drugs. The amount of money paid in consultation has nearly quadrupled since 2013. Results are consolidated in Table 1 and Figure 1.
Discussion
This past decade has been an exciting period in cancer research and drug approvals, with myeloma being one of the many malignancies benefitting from this progress. This was made possible by the collaboration between pharmaceutical companies and academic institutions. With the need for continuous combination therapy in multiple myeloma along with increasing prices of existing drugs and high upfront market prices for newly approved drugs, there is significant financial burden placed on the healthcare system. Based on the published literature substitution of carfilzomib for bortezomib or addition of monoclonal antibodies in induction would double cost. Some of these drug approvals are based solely on surrogate endpoints of overall response rates and progression free survival benefit of few months. This is without proven overall survival data while harboring significant toxicity.
Conclusion:
With pharmaceutical companies spending millions of dollars for drug development there has been a trend towards higher drug pricing. These companies also pay large amounts of consulting fees to physicians dedicated to aggressively market these newly approved drugs which are priced higher than existing therapy. Some of the current cancer guidelines include authors who have financial conflicts of interest and receive consulting fees from pharmaceutical companies. It would be interesting to investigate the correlation between the consulting fees and its effect on prescription patterns. Even the cancer care guidelines do not consider the cost effectiveness of equally effective regimens. There has been a push from various pioneers in the field to incorporate value-based recommends into their guidelines. Given the trajectory of rising costs within our healthcare system, it is imperative for all physicians to be mindful of value-based care while seeking therapy options that provide true benefit to their vulnerable patient populations.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal