

Background
Therapy related acute myeloid leukemia (t-AML) constitutes a subset of AML that has an increased proportion of high risk cytogenetic and molecular features, poor response to therapy, higher relapse, and decreased overall survival. The incidence ranges from 10-20% across various studies. Allogeneic hematopoietic stem cell transplantation (allo-HSCT) offers a potential cure in t-AML, with disease free survival reported up to 30% at 2 years. Most studies on HSCT in t-AML have limited number of patients and are confounded by the inclusion of patients with secondary AML and therapy related myelodysplastic syndromes (t-MDS). We aim to report our 20-year experience of allo-HSCT in t-AML and identify predictors of survival.
Patients and Methods
We retrospectively reviewed all cases of t-AML who underwent allo-HSCT at our centre from June 1999 to July 2019. We collected data for demographic characteristics, prior malignancy and treatment, latent period before AML, cytogenetic and molecular characteristics of AML, induction treatment received, transplant details (donor details, conditioning regimens, GVHD prophylaxis) as well as post-transplant complications (transplant related mortality, occurrence and severity of acute and chronic GVHD, CMV and EBV reactivations). Primary outcome evaluated was overall survival and secondary outcomes were relapse rate and relapse free survival (RFS). Cox-proportional hazards regression model was used to identify predictors of survival.
Results
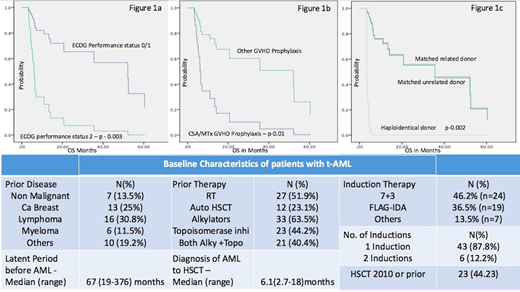
Fifty-two patients underwent allo-HSCT for t-AML during the study period. 58% were male (n=30). Median age at HSCT was 55.5 years (Range 18-70). Baseline characteristics are summarized in Table 1. Complex cytogenetics were present in 23.2% (n=12) patients, while 11q23 rearrangement (MLL-KMT2A), monosomy 7, monosomy 5, and 17p deletion were present in 15.4% (n = 8), 15.4% (n= 8), 7.7% (n = 4) and 7.7% (n=4) patients respectively. Based on the ELN 2017 risk stratification schema, 13.5% (n=7) patients could be considered favorable risk based on cytogenetic and molecular profiles, 36.5% (n=19) intermediate risk, and 57.7% (n=30) in poor risk category. Performance status prior to transplant was ECOG 0/1 in 71.2% (n=37) patients, and 2 in 28.8% (n=15) patients. Myeloablative conditioning was used in 30.8% (n=16) patients, and reduced intensity conditioning in 69.2% (n=36). GVHD prophylaxis was CyclosporineA(CSA)/Methotrexate in 23.1% (n=12), Alemtuzumab/CSA in 21.2% (n=11), ATG/CSA/PTCy in 28.8% (n=15), and other regimens in 26.9% (n=14) patients. Transplant related mortality (death before day+100) was 21.1% (n=11). Acute and chronic GVHD (any grade) occurred in 61.5% (n = 32) and 28.8% (n=15) patients respectively. Eleven patients (21.2%) relapsed with a median RFS of 8 months (Range 0.17-158). Median OS of the whole cohort was 8.9 months (0.17-158 months). No patient had a relapse of their primary malignancy during follow up. RFS at 12 and 24 months were 46% and 28% while OS at 1 and 2 years was 46% and 30%, respectively. Significant predictors of reduced OS (Figure 1a,b,c) after day+100 of HSCT by Cox-regression were ECOG performance status 2 (Hazard ratio - 6.1; p value 0.003), GVHD prophylaxis with CSA/methotrexate (HR - 4.5; p value 0.01), and haploidentical donor transplantation (HR - 34; p value - 0.002). Cytogenetics were a predictor of OS in univariate analysis but not in multivariate regression analysis. No difference in OS was found between patients who underwent HSCT 2010 or prior versus after 2010.
Conclusions
Patients with favorable cytogenetic profile, better performance status, and an HLA matched donor may have better outcomes after allo-HSCT in therapy related AML. Patients with unfavorable cytogenetic risk profiles may require more intense therapy or post-transplant maintenance therapy to prevent relapse.
Michelis:CSL Behring: Other: Financial Support. Mattsson:Gilead: Honoraria; Celgene: Honoraria; Therakos: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal