

Introduction:
Autologous stem cell transplant (ASCT) followed by maintenance is the standard of care for eligible patients with multiple myeloma (MM). For patients that relapse, a second ASCT remains a viable option. However, the maintenance regimen to use for such patients remains an unanswered question, particularly in those with prior lenalidomide exposure. We retrospectively analyzed patients receiving two autologous transplants for a diagnosis of MM at our institution from 2008 to 2018 to determine maintenance strategies and outcomes upon completion of a second transplant.
Methods:
A total of 189 patients received two or more autologous transplants for MM at our institution from 2008 to 2018. Patients with planned tandem transplants, or those that proceeded directly to another transplant without interval progression were excluded. The remaining 135 patients were analyzed.
Results:
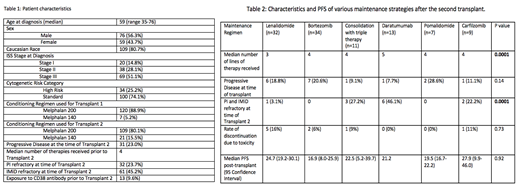
Patient characteristics are shown in Table 1. After first ASCT, 94 out of 135 patients (69.6 %) started maintenance therapy. The most commonly used maintenance regimen was lenalidomide in 63 patients, followed by bortezomib in 12 patients and thalidomide in 10 patients. Median time to initiation of maintenance from the date of transplant was 3.9 months. Overall median progression free survival (PFS) from transplant was 24.7 months with no significant difference between groups that received lenalidomide (median PFS: 21.2 months) or bortezomib (median PFS: 19.2 months, p:0.12). 10 (15.8%) patients discontinued lenalidomide due to toxicity, and 1 patient (8.3%) discontinued bortezomib due to toxicity.
The median time from the onset of disease progression post first ASCT to time of second ASCT was 5.8 months. Strategies used post second ASCT includedconsolidation with triplet regimens followed by de-escalation (n=11) versus monotherapy (n=100). Table 2 highlights differing maintenance regimens used after the second ASCT.
Median time from second ASCT to initiation of maintenance was 4.0 months. Median PFS post ASCT was 20.7 months. There was no statistically significant difference in PFS between the different regimens used (p=0.26), although there was a numerically higher discontinuation rate due to toxicity with older agents such as lenalidomide and bortezomib compared with newer agents such as daratumumab and pomalidomide. There was no statistically significant difference in the cytogenetic risk profile (p=0.21) or stage at diagnosis (p=0.36) between the groups that received different types of maintenance agents. However, patients receiving daratumumab as maintenance were more likely to have received more lines of therapy (median 5 for Daratumumab vs 3 for Lenalidomide, p=0.0001), and more likely to have previous exposure to daratumumab prior to second ASCT (92% vs 0% for other agents p=0.0001). Patients receiving daratumumab, carfilzomib or triple therapy were more likely to have been refractory to both a proteasome inhibitor (PI) and an immunomodulatory drug (IMiD) (p=0.0001).
Despite stratifying for use of newer novel drugs (FDA approval after 2010- pomalidomide, daratumumab, carfilzomib) vs older novel drugs (FDA approval before 2010- lenalidomide, bortezomib, thalidomide), there was no difference in PFS ( 21.2 months vs 20.4 months, p= 0.92), between these groups when used as part of a maintenance strategy.
Conclusions:
Our data show a variety of maintenance and consolidation regimens are used for patients with MM after their second ASCT. In this single-center, retrospective analysis, there was no clear superiority of a consolidative strategy using triplet over monotherapy, and no superiority of newer agents compared to older agents. This suggests that toxicity, prior therapies and their tolerance may be the more important patient-related factors for consideration when selecting an agent/agents. Randomized, prospective data will be important to ascertain the standard of care in this situation.
Ganguly:Daiichi Sankyo: Research Funding; Seattle Genetics: Speakers Bureau; Kite Pharma: Honoraria, Other: Advisory Board; Janssen: Honoraria, Other: Advisory Board. McGuirk:Kite Pharmaceuticals: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Bellicum Pharmaceuticals: Research Funding; Astellas: Research Funding; Juno Therapeutics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Research Funding; Fresenius Biotech: Research Funding; Gamida Cell: Research Funding; Pluristem Ltd: Research Funding; ArticulateScience LLC: Other: Assistance with manuscript preparation.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal