

Introduction:
Frequent blood testing in the intensive care unit (ICU) is instrumental to patient diagnosis, monitoring, and titration of invasive therapies. However, there is a growing appreciation that a significant proportion of ICU blood tests are reflexive and unnecessary.1,2 Serial phlebotomy is associated with extended hospital length of stay and acquired anemia in the general hospital population.3 Since patients in the ICU are prone to developing anemia,4,5 they are likely at increased risk of harm from serial phlebotomy. In response, multiple recent campaigns advocate for physician restraint in laboratory test ordering.6,7 However, relatively little is known about the effect of excessive phlebotomy on outcomes in critically ill patients. Better understanding of ICU phlebotomy practices, and harms associated with serial testing, is important in planning, implementing, and evaluating phlebotomy reduction interventions.
Objectives:
1) Quantify average daily phlebotomy volume for ICU patients including blood discarded as waste when accessing vascular devices. 2) Identify if average daily phlebotomy volume is an independent risk factor for ICU acquired anemia (hemoglobin < 80 g/L) or the need for red blood cell transfusion. 3) Explore the relationship between daily phlebotomy volume and hospital mortality.
Methods:
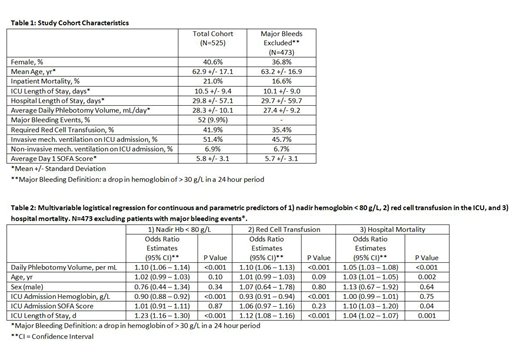
This was a retrospective cohort study at an academic tertiary care center in Toronto, Ontario, utilizing hospital administrative data, laboratory data, and select chart review. Index Medical Surgical ICU admissions between September 2014 and August 2015 with an ICU stay of three days or greater were included. Major bleeding events were defined as a hemoglobin drop of 30 g/L within a 24 hour period. Average daily phlebotomy volumes were calculated using the number of samples received by the lab multiplied by standard blood volumes required for each sample type. A bedside prospective audit was conducted in March 2018 to quantify average blood volume discarded as waste during phlebotomy. Blood discard/waste data were summarized with descriptive statistics, but not included in further analysis. Multivariable logistic regression was used to study the association between average daily phlebotomy volume and each of: nadir hemoglobin (< 80 g/L), the need for red blood cell transfusion, and hospital mortality. Patients with a major bleeding event were excluded from the regression. Control variables included sex, age, ICU length of stay, admission hemoglobin, and admission Sequential Organ Failure Assessment (SOFA) score.
Results:
There were a total of 525 index patient admissions, mean age 62.1 yr, 41% female (Table 1). Fifty-two (52) patients had a major bleeding event in the ICU. Mean phlebotomy volume per patient day was 28.3 mL (95% CI 27.4 - 29.1 mL, stdev 10.1 mL). Mean bedside waste during the phlebotomy audit (total of 144 blood draws) varied by vascular access: 3.9 mL for arterial, 5.5 mL for central venous, and 6.25 mL for peripherally inserted catheters. The mean estimated daily bedside waste for phlebotomy was 14.8 mL per patient day. Outcomes of logistical regression, excluding patients with major bleeding events, are summarized in Table 2. Average daily phlebotomy volume (mL) was predictive of nadir hemoglobin < 80 g/L (parameter estimate 0.091, p <0.001), the need for red blood cell transfusion (0.092, p<0.001), and inpatient mortality (0.053, <0.001). For every 5 mL increase in average daily phlebotomy, the odds ratio (OR) for nadir hemoglobin < 80 g/L was 1.58 (95% CI 1.31 - 1.90) and the OR for a red cell transfusion was 1.58 (95% CI 1.33 - 1.87).
Conclusion:
Daily ICU phlebotomy volume is associated with ICU acquired anemia and the need for red blood cell transfusion, including in a multivariable model with patient demographics, major bleeding events, and severity of illness as estimated by day 1 SOFA score. However, the ICU admission SOFA score was only weakly predictive of mortality, and the unexpected association between average daily phlebotomy and mortality needs to be further explored. It is possible that in this data set day 1 SOFA score did not completely control for severity of illness. Our findings support the need for ongoing phlebotomy stewardship interventions in the ICU. We suggest ICU acquired anemia and the need for red blood cell transfusion are appropriate patient outcome measures to evaluate stewardship interventions.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal