

Introduction
Multiple myeloma has relished the emergence of various novel agents in last few decades. Unfortunately,relapses are still an inevitable part and at each relapse, treatment choice becomes a complex decision making process as these patients usually have exhausted conventional therapeutic regimens.Carfilzomib is a second-in class Proteosome Inhibitor (PI) and has been approved for patientsrefractory to minimum 2 lines of prior therapies. We are, hereby, presenting our initial experience with this novel combination (KPD)in RRMM patients at our centre.
Methodology
Retrospective study of RRMM patients who received KPD therapy from August 2017 till October 2018. Responses were assessed as per International Myeloma Working Group. Study was approved by Institutional Review Board.
Results
Total 39 patients were treated with KPD regimen during study period. Median age was 56 (32-74 years) with male ratio of 51.2% (n=20). At baseline presentation, bone disease {n=32 (82%)} was the most common presenting complaint followed by anemia {n=21 (53.8%)} and renal failure {n=16 (41%)}. Most common ISS staging was ISS-3 {n=18(46.1%)} and subtype was Light chain myeloma {n=15 (38.3%)} followed by IgG {n=13 (33.3%)}.Fluorescence In Situ Hybridization (FISH) was available in {n= 10 (25%)} and it was positive for del13q (n=1/10) and del17p (n=1/10) and t(11;14) (n=1/10). (Table-1)
Median number of prior lines of chemotherapy was 3(1-15). Thirty-six (91%) patients were relapsed/refractory to both bortezomib and lenalidomide whereas n=3(9%) were relapsed/refractory to bortezomib only. Eleven (30.5%) patients underwent SCT pre KPD therapy including 2/11 patients received double SCT. Pre KPD 25 (64.1%) patients had progressive disease (PD), 10 (25%) had relapse and 4 (11.1%) patients had stable disease (SD).
Median number of KPD cycles were 3(1-8). Median number of KPD cycles after which response assessment was donewas 3 (2-8). Median time to treatment response was 3 (2-7) months. ORR was 51.2% {CR-n=5 (12.8%); VGPR-n=5 (12.8%), PR-n=10 (25.6%)} whereas 2 (5.1%) patient had SD and 10 (25.6%) patients had PD at 2-8 cycles. Two (5.1%) patients are yet to be assessed. (Table-1)
Common hematological toxicities seen were anemia (n=8), thrombocytopenia (n=13){grade-3/4=30.7%; n=4/13} and neutropenia(n=14){grade3/4=21.4%; n=3/14}.Non haematological toxicity such as cardiac toxicity was not observed in our patients. Pre KPD 2D-ECHO was available for 13 patients and which was normal in all patients. Post 2-4 cycles of KPD, 2D-ECHO was available for 7 patients and all patients had normal ECHO. Carfilzomib induced hypertension was seen in 20 patientsand could be well controlled with antihypertensives. Peripheral neuropathy (grade1/2) was seen in 10 patients. We also observedCarfilzomib induced hyponatremia in one patient.Febrile neutropenia(bacterial =6, viral=4, possible fungal=5) was seen in 14 patients.(Table-2)
Twelve (20.5%) patients proceeded to either maintenance therapy or autologous stem cell transplantation (ASCT). Eight patients opted only for maintenance (carfilzomib=5, pomalidomide-dexamethasone=2 and pomalidomide =1). Remaining n=4/12(16%) patients received SCT. Pre SCT response status was VGPR n=2; PR n=1 and SD=1. Post SCT response status was VGPR (n=3) &PR (n=1). Post SCT, 3 patients were started on maintenance therapy as Bortezomib/pomalidomide=1, Pomalidomide/dexamethasone=2. One patient has been continued on KPD as a consolidation therapy.
At a median follow-up of 10 months (1-14 months), relapse rate was 12.8% (n=5). Ten (25.6%) patients had PD.Mortality rate was 8.3% (n=3), commonest cause being progressive disease.
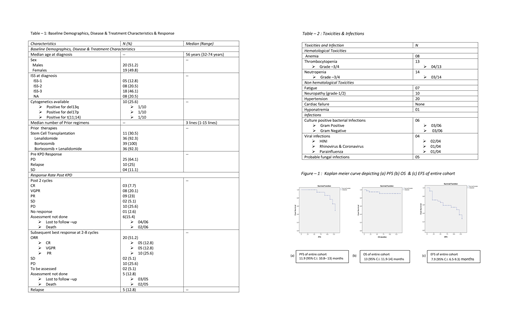
The estimated mean PFS, OS and EFS of entire cohort was 11.9 months (95% C.I. 10.8- 13 months) (figure-1 a), 13 months (95% C.I. 11.9-14 months) (figure-1 b) and 7.9 months (95% C.I. 6.5-9.3 months) (figure - 1 c) respectively.
Conclusion
KPD is a well-tolerated regimen for patients with RRMM who have exhausted frontline myeloma regimen, however at the cost of significant side effects like infections and hypertension. It seems to be a convincing regimen as a bridge to ASCT but warrants further studies with longer follow-up to validate our results.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal