

Introduction
Lenalidomide (Len) and low-dose Dexamethasone (dex) (Rd) in continuous is a new standard of care for elderly newly-diagnosed multiple myeloma (NDMM) patients (pts), as established by FIRST trial (Facon et al, Blood 2018).
Methods and results
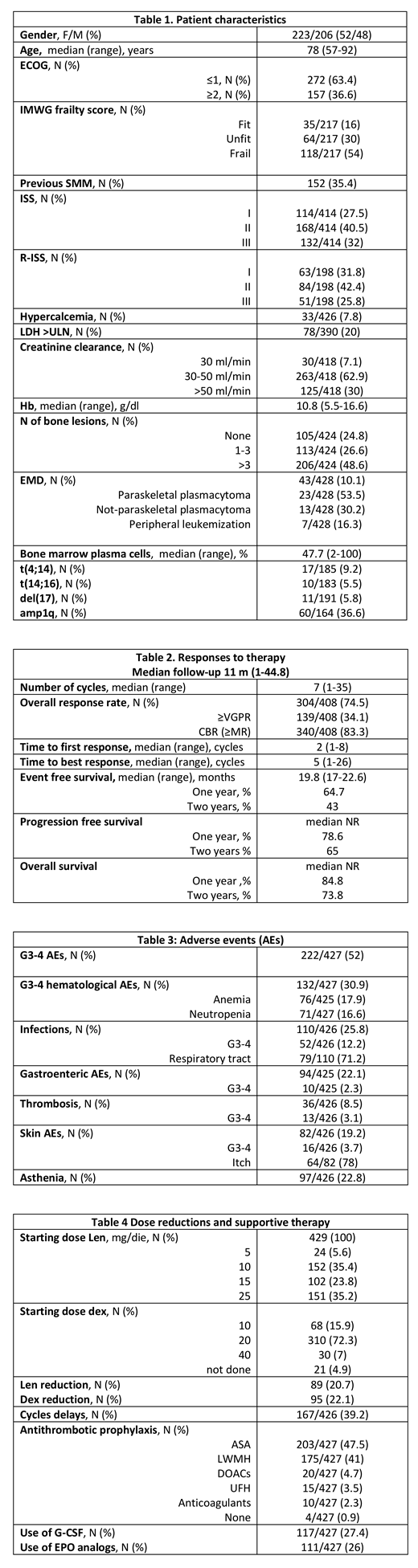
This is a retrospective, multicentric study conducted in Italy with the aim of evaluating efficacy and tolerability of Rd in a real-life population. Thirty-seven centers were involved and data of 429 pts are available. Pts were considered eligible for the study when completing at least 2 cycles of Rd regimen. Table 1 summarizes the characteristics of pts at time of MM diagnosis. Median age was 78 years (range 57-92), 36.6% had an ECOG PS≥2, creatinine clearance (ClCr) was <30 ml/min in 7.1% of pts. 16, 30 and 54% resulted respectively fit, unfit and frail by IMWG Frailty score. ISS was respectively I, II and III in 27.5, 40.5 and 32% while R-ISS was I, II and III in 31.8, 42.4 and 25.8% of pts. t(4;14), t(14;16), del(17p) or amp(1q) by FISH were respectively found in 9.2%, 5.5%, 5.8% and 36.6% of pts. Extramedullary disease (EMD) was documented in 11% of pts.
After a median follow-up of 11 months, most pts are still on treatment (60,4%), the median number of administered cycles was 7 (range 2-33).
Overall response rate (ORR, ≥PR) was 74.5% with 34.1% of pts obtaining at least a VGPR. Clinical Benefit Rate (CBR, including minimal responses) was 83.3%. Responses were rapid with median time to first and to best response respectively of 1.8 (range 1-8) and 5 (1-26) months. Median OS and PFS were not reached with a 1-y and 2-y OS of 84.8 and 73.8% and a 1-y and 2-y PFS of 78.6 and 65%. Median EFS was 19.8 months.
In univariate analysis, factors significatively impairing ORR were frailty (fit/unfit/frail 91.2/77/55.9%, p<0.001), ECOG (0-1/>2 81.7/61.6%, p<0.001), presence of t(4;14) (52.9 vs 76.7%, p=0.033) and amp(1q) (53.4 vs 83.5, p<0.001), R-ISS (3 vs 2-1 55.3 vs 72.6%, p=0.027), LDH > upper level of normal (ULN) (65.8 vs 77%, p=0.034). 1-y PFS is significantly shorter in pts with lower ECOG (0-1 vs 2, 66.5 vs 84.8%, p<0.001), higher frailty score (fit/unfit/frail 100/86.4/66.6%, p=0.01), higher ISS (I-II-III 88.4-79.1-68.5%, p=0.002) and R-ISS (I-II-III 75.5-88-50.5% p=0.02), LDH >ULN (66.4 vs 83.2%, p=0.02), lower ClCr (<30/30-50/>50 57.2/81.3/80.1%, P=0.01), presence of t(14;16) (42.9 vs 80.4% p=0.01) and amp(1q) (63.5 vs 85.6%, p=0.01); factor impairing OS are ECOG (0-1/>2 93.4 vs 69.4%, p<0.001), frailty (fit/unfit/frail 100/90.5/75.3% p=0.001), higher ISS (I-II-III 93.6/87.8/74.6%, p=0.006) and R-ISS (I-II-III 87/93/72%, p<0.001)), LDH >ULN (75.1 vs 97.1, p=0004), impaired ClCr (<30/30-50/>50 64/83.7/88.2%, p<0.001); EFS was affected by ECOG (0-1/>2 74.2 vs 47.3%, p<0.001), frailty (fit/unfit/frail 83.4/74.5/52% p=0.09), R-ISS (I-II-III 61.4/74.9/37.5% p=0.006), presence of t(14;16) (35.5 vs 67.8% p=0.08) or amp(1q) (50.1 vs 69% p=0.02).
In multivariate analysis ORR is significantly correlated with ECOG>2 (p=0.05), LDH >ULN (p=0.005) and presence of amp1q (p=0.006); PFS was significantly affected by R-ISS III (p=0.04), LDH >ULN (P=0.01) and ClCr<30 (p=0.006) and EFS by R-ISS III (p=0.002); only ECOG>2 still impact on OS (p<0.0001)
Dose reduction of Len or dex was required respectively in 20.7% and 22.1% and 39.2% needed cycle delay for adverse events (AEs). Grade 3-4 (G3-4) AEs occurred in 52% of pts with 30.9 and 36.6% having at least a hematological or extra-hematological G3-4 AE. In particular, 17.9 and 16.6% of pts had severe neutropenia and anemia while the most common non-hematological AEs were infections (25.8%, G3-4 12.2%), mainly involving respiratory tract (71.2%). Gastroenteric and cutaneous AEs were quite common (22.1 and 19.2%), mainly diarrhea and itching, but in the vast majority were mild. G3-4 asthenia was present in 22.8% of pts. Although 99% of pts was given antithrombotic prophylaxis, 8.5% had a thromboembolic event, a third of severe entity. G-CSF and EPO analogs were required in 27.4 and 26% of pts.
Conclusion
Real-life data confirm efficacy and tolerability of Rd in elderly NDMM pts. Performance status by ECOG and IMWG frailty score and severe renal impairment but not age itself act as limiting factors affecting outcome. These data must be confirmed by longer follow-up.
Conticello:Celgene: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding. Mangiacavalli:Janssen cilag: Consultancy; celgene: Consultancy; Amgen: Consultancy. Zambello:Celgene: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees. Belotti:Amgen: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees. Molteni:Celgene: Membership on an entity's Board of Directors or advisory committees. Aquino:Celgene: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees. Del Fabro:Janssen: Consultancy. Galli:Leadiant (Sigma-Tau): Honoraria; Janssen: Honoraria; Bristol-Myers Squibb: Honoraria; Takeda: Honoraria; Celgene: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal