

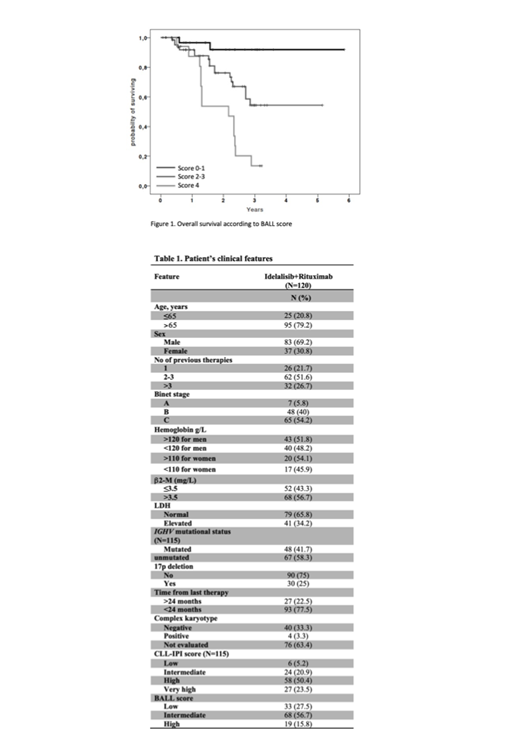
The CLL-IPI score, which combines genetic, biochemical, and clinical parameters, represents a simple worldwide model able to refine risk stratification for CLL patients. This score, developed in the era of chemo-immunotherapy, has not been gauged extensively in R/R-CLL patients treated with novel targeted agents, such as BCR and BCL2 inhibitors. Soumerai et al (Lancet Hematol 2019) assembled a novel risk model for OS in the setting of R/R-CLL receiving targeted therapies in clinical trials. This model, consisting of four accessible markers (β2M, LDH, Hb, and time from initiation of last therapy; BALL score), is able to cluster 3 groups of CLL patients with significantly different OS. This multicenter, observational retrospective study aimed to validate the proposed Soumerai (BALL) and/or CLL-IPI scores for R/R-CLL real-world patients treated with idelalisib and rituximab (IDELA-R). The primary objectives were to determine whether: i) the CLL-IPI retains its prognostic power also in R/R patients treated with IDELA-R; ii) the BALL score is of prognostic value for IDELA-treated R/R-CLL patients, and iii) the BALL score is predictive of PFS. This study, sponsored by Gilead (ISR#IN-IT-312-5339), included CLL patients collected from 12 Italian centers, who received IDELA-R (idelalisib 150 mg b.i.d. and a total of 8 rituximab infusions intravenously) outside clinical trials as salvage therapy with available data for the calculation of the CLL-IPI and BALL scores at the time of treatment start. OS was estimated for all subgroups of both scores. Additionally, risk-specific PFS was assessed. Kaplan-Meier curve, log-rank test, and Cox regression analyses were performed. The prognostic accuracy of the predictive model was assessed by Harrell's C-index. Overall, 120 CLL patients were included in this analysis. The majority of patients were Binet stage B and C (94.2%). The median age was 75 years and 83 cases (69.2%) were male. The median number of previous therapies was 3 (range 1-9) Baseline patient features are listed in Table 1. After a median follow-up of 1.6 years (1 month to 5.8 years), 33 patients had died and 39 experienced an event (death or progression). CLL-IPI scoring (115/120 evaluable cases) indicated that 6 patients (5.2%) were classified as low-risk, 24 (20.9%) as intermediate-risk, 58 (50.4%) as high-risk, and 27 (23.5%) as very high-risk. Stratification of patients according to the CLL-IPI score did not allow prediction of significant differences in OS. Thus, low-risk patients had a 2-year OS probability of 75% (HR=1), with an intermediate-risk of 68% (HR=2.9, 95%CI 0.37-23.3, P=0.3), high-risk of 83% (HR=1.58, 95%CI 0.2-12.5, P=0.66), and very high-risk of 63% (HR=5.9, 95%CI 0.78-45.2, P=0.86). Next, we tested a modified CLL-IPI by assigning a more balanced score to the original CLL-IPI variables (Soumerai et al, Leukemia Lymphoma 2019), partially overlapping previous results. Specifically, modified CLL-IPI high-risk group showed a significantly different OS as compared with intermediate- and low-risk groups. However, differently from the original report no difference was observed between low- and intermediate-risk). According to the BALL score (120/120 evaluable cases), 33 patients (27.5%) were classified as low-risk, 68 (56.7%) as intermediate-risk, and 19 (15.8%) as high-risk. Stratification of patients according to the BALL score predicted significant differences in terms of OS. Thus, low-risk patients had a 2-year OS probability of 92% (HR=1), intermediate-risk of 76% (HR=5.47, 95%CI 1.3-23.7, P=0.023), and high-risk of 54% (HR=15.1, 95%CI 3.4-67, P<0.0001) (Figure 1). Harrell's C-statistic was 0.68 (P<0.001) for predicting OS. To note, BALL score failed to significantly stratify patients in terms of PFS. As for Soumerai et al (Leukemia Lymphoma 2019), the original CLL-IPI score did not retain discriminative power in term of OS in R/R-CLL patients receiving IDELA-R. The modified CLL-IPI failed to stratify low- and intermediate-risk groups, likely due to the number of cases analysed in the current cohort and the heterogeneous IDELA-containing regimens included in the Soumerai study (Soumerai et al, Leukemia Lymphoma 2019). The CLL-IPI was designed for CLL patients treated with first-line chemo-immunotherapy. Herein, we confirm the prognostic power of the BALL score in this real-world series for OS, while losing the predictive impact of patient outcomes in terms of PFS.
Mauro:Gilead: Consultancy, Research Funding; Jannsen: Consultancy, Research Funding; Shire: Consultancy, Research Funding; Abbvie: Consultancy, Research Funding; Roche: Consultancy, Research Funding. Coscia:Abbvie: Membership on an entity's Board of Directors or advisory committees; Gilead: Membership on an entity's Board of Directors or advisory committees; Karyopharm Therapeutics: Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding. Varettoni:ABBVIE: Other: travel expenses; Roche: Consultancy; Janssen: Consultancy; Gilead: Other: travel expenses. Rossi:Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Abbvie: Honoraria, Other: Scientific advisory board; Janseen: Honoraria, Other: Scientific advisory board; Roche: Honoraria, Other: Scientific advisory board; Astra Zeneca: Honoraria, Other: Scientific advisory board. Gaidano:AbbVie: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Sunesys: Consultancy, Honoraria; Astra-Zeneca: Consultancy, Honoraria; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal