

Background: Azacitidine is the current standard of care for higher risk MDS patients (HR MDS) changing the natural course of diseases. Early drug discontinuation (receiving less than 4 azacitidine cycles - early failure - EF) is a poor prognostic marker, while factors affecting early failure are largely unknown.
Objectives: To identify predictive factors for early azacitidine failure in MDS/CMML/low blast percentage AML patients
Methods: The study included retrospectively MDS/CMML and 20-30% bone marrow blasts AML patients treated from 2008 to 2019 in 12 Polish hematologic centers cooperating within Polish Adult Leukemia Group (PALG). Baseline demographic, laboratory, clinical and treatment characteristics were obtained and were evaluated as potential EF predictors. Cox proportional hazard models were used to define statistical significance of variables using the R statistical platform.
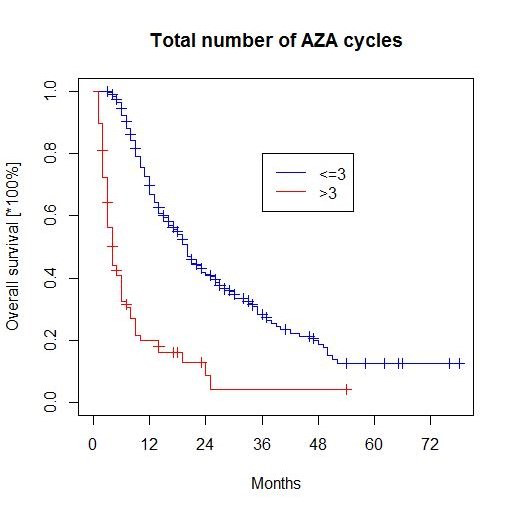
Results: We collected data on 315 patients with MDS (67%), CMML (12%) and with AML (21%). Median age was 69 years and 61% were male. Median number of azacitidine cycles was 7 (1-69) and 84 patients (29%) received maximum 3 cycles. Patients achieved more than 3 cycles showed better OS compared to those ≤ 3 cycles (20 months vs 4 months)(p<0.05)( Figure 1). In univariate analysis the following features were significantly predictive for early failure: poorer cytogenetics IPSS (OR 1.87, 95% CI 1.36-2.56; p<0.001), poorer cytogenetics IPSS R (OR 1.52, 95% CI 1.21-1.89; p< 0.001), poorer IPSS score (OR 1.77, 95% CI 1.18-2.66; p0.006), poorer ISS R score (OR 1.51, 95% CI 1.07-2.14; p=0.02), earlier treatment (OR 2.43, 95% CI 1.33-4.44; p=0.004), serum albumin level (OR 0.44, 95% CI 0.27-0.74; p=0.002), coexistence of autoimmune disease (OR 1.49, 95% CI 1.12-1.99; p=0.007), ECOG performance status (OR 1.49, 95% CI 1.12-1.99, p=0.007) and ativiral prophylaxis management (OR 0.40, 95% CI 0.19-0.87, p=0.020). In the multivariate analysis only serum albumin level retained its significance as independent factor affecting the risk of EF (OR 0.30, 95% CI 0.13-0.7; p=0.005). Decrease of albumin level by 1 g/dL rises the risk of EF occurence by 70%.
Conclusions: Our analysis confirmed that patients with premature azacitidine treatment discontinuation ≤ 3 cycles have worse outcome. The pretreatment lower serum albumin level was identified as an independent predictor of early failure occurence.
Figure 1. Overall survival in patients treated with ≤ 3 azacitidine cycles and > 3 cycles
Golos:Novartis: Honoraria. Basak:Celgene: Honoraria; Teva: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal