

We are reporting a challenging case 37-year-old Pakistani male patient with Hepatosplenic T-Cell lymphoma (HSTCL) which is a rare aggressive form of Peripheral T-Cell lymphoma that is characterized by primary extra nodal disease with malignant T-cell proliferation in the liver, spleen, and bone marrow. He presented initially with nonspecific symptoms of generalized fatigue & vague abdominal pain . He was found to have hepatosplenomegaly (with liver & splenic lesions), derranged liver enzymes. He refused investigation and lost follow up.
He came back 3 months after in a bad condition with fever, abdominal pain & he deteriorated very rapidly. The diagnosis was challenging as he required an extensive investigations that ultimately showed the characteristic clinical, histopathologic, and cytogenetic features of hepatosplenic T-cell lymphoma with HLH presentation.
Patient had multiorgan failure,coagulopathy, shock(hepatic/renal/septic) and started on vasopressors, Ferritin was high >16000, Secondary Hemophagocytic Lymphohistiocytosis (HLH) was made at this point & patient was started on dexamethasone as per HLH protocol 2004 to reduce the tumor burden, and the plan was to start CHOP after 2 days, if patient condition allowed.
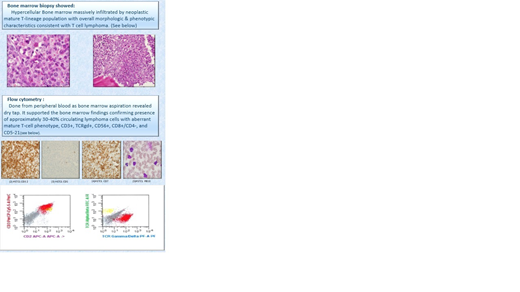
Bone marrow biopsy showed: hypercellular Bone marrow massively infiltrated by neoplastic mature T-lineage population with overall morphologic & phenotypic characteristics consistent with T cell lymphoma.
Flow cytometry was done from peripheral blood as bone marrow aspiration revealed dry tap.it showed presence of approximately 30-40% circulating lymphoma cells with aberrant mature T-cell phenotype, CD3+, TCRgd+, CD56+, CD8+/CD4-, and CD5-. The overall morphology and immunophenotypic features were consistent with hepatosplenic T-cell lymphoma (WHO classification updated 4th edition,2016).
patient received full CHOP. All through patient was steadily worsening and unfortunately passed away.
HSTCL is a rare and challenging diagnosis and presentation can be dramatic like this case with HLH. T cell lymphoma can present with HLH and treatment
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal