

Accurately distinguishing between mature and immature B-cell neoplasms is crucial for determining therapy. However, overlapping morphologic, cytogenetic and immunophenotypic characteristics can have diagnostic and therapeutic implications. Morphologically, high grade B-cell lymphoma with double/triple hit (HGBL) may have a "starry sky" or blastoid appearance that can resemble B-lymphoblastic leukemia (B-LBL), Burkitt's Lymphoma (BL) or diffuse large B cell lymphomas (DLBCL), but differ from immature B-cell neoplasms with expression of CD20, CD10, MUM1, and surface immunoglobulin light chains (sIG). Conversely, B-LBL and B-ALL lymphoblasts have dim or lack expression of CD20 and sIG and express markers of immaturity such as CD34 and terminal deoxynucleotidyl transferase (TdT). In this study, we present our institutional experience of 8 patients with a "grey zone" leukemia/lymphoma: 4 patients with aggressive TdT-positive HGBL and 4 patients with B-LBL or B-ALL with a "double-hit" karyotype. We hypothesize these cases may represent a separate entity between HGBL and B-LBL/B-ALL with activating Myc rearrangements.
Our cohort was compiled by reviewing cases encountered in our clinical practice from July 2015 to July 2019 that could be identified as follows: (1) de novo HGBL with MYC, BCL2, and/or BCL6 rearrangements or amplifications with concurrent aberrant TdT expression at diagnosis or in subsequent biopsies and (2) de novo B-LBL or B-ALL with a "double‐hit" karyotype. Clinical and diagnostic data were obtained by review of the medical records. The Moffitt Cancer Center Institutional Review Board approved this retrospective study.
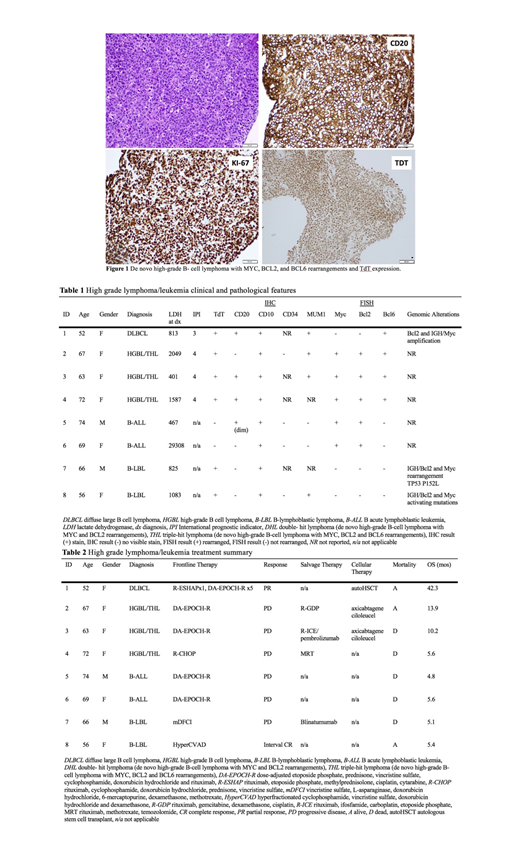
Of patients with HGBL with aberrant TdT expression, 3 were HGBL with triple hit and 1 with a Bcl6 rearrangement and Bcl2 and Myc amplifications. These patients presented with aggressive features including elevated LDH at diagnosis, high IPI score, and Ki-67 >/= 80%, however without bone marrow or CNS involvement. They express a typical GCB immunophenotype, positive for CD10, CD20, and MUM1 and negative for CD34 (Table 1). These patients were treated with DA-EPOCH-R (3) and R-CHOP (1), of which 1 achieved a partial response and 3 developed progressive disease (Table 2). Three patients went on to consolidative therapy with CD19-directed CAR-T (66%) or autologous transplant (33%). The median overall survival (mOS) was 12.1 months. In the second group, 2 were considered B-ALL based on immature morphology and lack of mature B-cell markers (CD20 negative or variable and MUM1 negative), although they did not express TdT. They both showed IGH-Bcl2 and Myc rearrangements. They were treated with DA-EPOCH-R, of which 1 experienced progressive disease and 1 was unable to complete therapy. The other 2 patients were diagnosed with de novo B-LBL that was CD10 and TdT positive. Of these, 1 showed MUM1 positivity and genomic testing revealed IGH-Bcl2 and Myc rearrangements accompanied by a TP53 mutation. The other showed IGH-Bcl2 rearrangement and Myc activating mutation. One was treated with HyperCVAD with an interval CR and the other with modified DFCI died 5.1 months after diagnosis. Prognosis in this second subset was poor with a mOS of 5.3 months. Within the entire cohort, the majority (75%) were treated as DLBCL with R-CHOP-based therapy, while the remaining (25%) were treated with HyperCVAD. 25% experienced a PR or interval CR, while the remainder experienced progressive disease (PD). Overall, we observed a median PFS of 6.6 months and mOS 5.6 months with 0% undergoing allogeneic transplant in first remission, 1 (12.5%) undergoing autogeneic transplant in first remission and 2 (25%) undergoing CD19-directed CAR-T following salvage therapy.
HGBL that has acquired TdT expression and B-LBL/B-ALL associated with IGH/BCL2 translocation and activating MYC rearrangements or mutations are uncommon, but represent a biologically unique group with a poor clinical outcome, likely due to accumulated somatic hypermutations. The high percentage of MUM1 expression in these cases suggests a role of dysregulated MUM1 in cooperation with Myc dysregulation. The recognition of this group may be under-appreciated due to the lack of awareness. Inclusion of evaluation of TDT in "mature" HGBL and identification of genetic alterations including BCL-2, BCL-6 and Myc in "immature" B-LBL/B-ALL will be helpful. Consolidation upon first remission with transplant or CAR-T may be of benefit.
Chavez:Genentech: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Kite: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Karyopharm: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees; Bayer: Membership on an entity's Board of Directors or advisory committees. Bello:Celgene: Speakers Bureau. Bunting:Transenterix: Equity Ownership; Tilray: Equity Ownership; Crispre: Equity Ownership; Celgene: Equity Ownership. Shah:Kite/Gilead: Honoraria; Adaptive Biotechnologies: Honoraria; AstraZeneca: Honoraria; Novartis: Honoraria; Spectrum/Astrotech: Honoraria; Incyte: Research Funding; Jazz Pharmaceuticals: Research Funding; Pharmacyclics: Honoraria; Celgene/Juno: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal