

Background:
According to the 2016 revised World Health Organization (WHO) Classification of Lymphoid Tumors, high grade B-cell lymphoma (HGBL) has been delimited as a new category with two subgroups: HGBL with rearrangements of MYC and BCL2 and/or BCL6 (so-called "double/triple hit lymphoma), and HGBL-NOS (HGBLs with features intermediate between DLBCL and Burkitt lymphoma). Retrospective data indicated many patients with HGBL diagnosed at an advanced stage and often have extremely poor outcome even if they received intensive chemotherapy. The accurate genetic and pathological mechanism of this high-risk lymphoma remains uncertain. For HGBL, traditional scoring may not be systematic enough and has limited reference value, more accurate prognostic grouping indicators are needed. The aim of this study was to evaluate the clinicopathological significances in newly diagnosed HGBL and DLBCL. Several clinical and hematological indexes in concert with Fluorescence in situ hybridization (FISH) rearrangement and Immunohistochemistry (IHC) expression profiles of biomarkers between HGBL and DLBCL will also be analyzed.
Methods:
We reviewed 52 patients diagnosed as HGBL or DLBCL in our hospital from 2017 to 2018 retrospectively. The clinical and hematological characteristics of the patients including age, gender, Ann-Arbor stage, B symptoms, serum LDH levels, β2-microglobulin (β2-MG), peripheral EBV-DNA copies, white blood cell (WBC), absolute neutrophil count (ANC), absolute lymphocyte count (ALC), and IPI score were collected. FISH detection was done in each patient to identify whether the patient had MYC, BCL2, and BCL6 rearrangement. The expressions of the above three indexes were done by IHC as well. NLR (neutrophil to lymphocyte ratio) was definited as ANC/ALC ratio.
Results:
A total of 52 newly diagnosed patients were included in this study, including 34 (65.4%) males and 18 (34.6%) females. The median age at diagnosis was 54.1 years old (range, 15-88 years), and 22 (42.3%) of them were more than 60 years old. Six patients were classified into the HGBL category and 2 of them were HGBL-NOS subgroup. Twenty-five patients were MYC, BCL2, or BCL6 rearrangement single-positive. Among them, MYC, BCL2, and BCL6 rearrangement were detected in 13.5%, 7.7%, and 30.8% of 52 patients respectively.MYC (cut-off value >40%), BCL2 (cut-off value >50%), and BCL6 expression was found in 48.1%, 50%, and 65.4% of 52 patients, respectively.
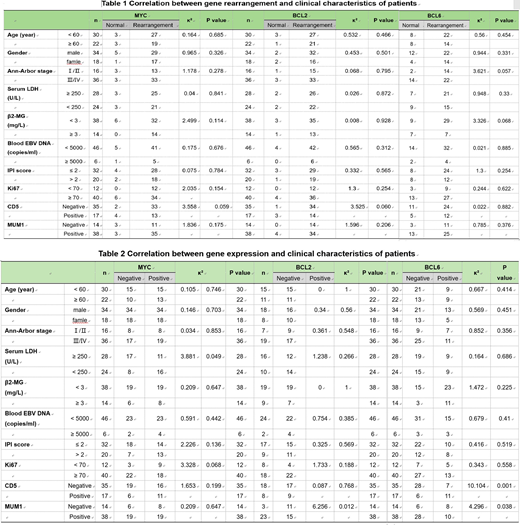
Among all of the patients, 32.7% (17/52) CD5 positive and 73.1% (38/52) MUM1 positive. 30.8% (16/52) of them were at stage Ⅰ/Ⅱ and 69.2% (36/52) of them were at stage Ⅲ/Ⅳ. 53.8% (28/52) of the patients had a high blood LDH level, 26.9% (14/52) showed an elevation of β2-MG level (>3mg/L) and 38.5% (20/52) presented high IPI score (IPI>2). The baseline clinical, hematological, and pathological characteristics are described in Table 1, 2.
3. With Pearson's Chi-square Tests analysis, the IPI score was significantly higher in patients older than 60 years old (P<01). Patients with the rearrangement of both BCL2 and BCL6 as well as CD5+ tend to have a higher Ki 67 ratio (P=0.045) and the same thing happened to patients with both MYC and BCL6 expression (P=0.049).
By the combination of either a positive gene rearrangement or a positive IHC marker (CD5 or MUM 1), there was a close association between any of the above with high β2-MG (P=0.024) and pheripheral EBV DNA copoies (P=0.012). Besides, the triple positive rearrangements combined with CD5 positive is associated with a higher NLR (P=0.027).
Conclusions:
In this study, we validated the prognostic value of several clinical, hematological, genetic, and pathological indexes in newly diagnosed HGBL and DLBCL. We found that if there's only one rearrangement gene or IHC marker (CD5 or MUM 1) positive, there was no significant difference between these alterations and some classic evaluation indexes such as serum LDH and Ann-Arbor stage. Patients with BCL2 + BCL6, or MYC + BCL6, or triple positive arrangement might have a more aggressive disease progression if positive CD5 expression could be detected at the same time. In the future, we plan to further evaluate if NLR has any correlation with the clinical outcome of patients with double-/triple-hit lymphomas or double-/triple expression lymphomas. More data from larger patient subset are needed to corroborate these findings.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal