

Introduction
Diffuse Large B-cell Lymphoma(DLBCL) is the most common type of Non-Hodgkin's Lymphoma, accounting for approximately 30% of adult lymphomas. Survival among patients with DLBCL has improved significantly in past years with the introduction of effective treatment modalities including Rituximab. Despite of improvement of survival, many patients undergo course of early death and disparities related to early death in DLBCL remains unclear. Our study was aimed to identify the characteristics and associated factors in patients with early mortality by retrospective study using a single-institutional patient data. The institution is a community hospital serving medically underserved population in urban setting, which is a unique setting to address disparities study.
Study design
Dataset was obtained from the institutional cancer registry and retrospective chart review. Patients diagnosed with biopsy proven DLBCL between January 2007 to December 2017 were included. Survival data was updated in July 2019. A total of 159 patients were included. Median survival was 99.5 months. Overall 2-year survival was 60.4% in all included patients. 90-day and 180-day mortality was defined as patients who survived less than 90 days or 180 days from diagnosis. Chi-square test was used for descriptive statistics. Cox-proportional hazard regression was used for survival analysis.
Result
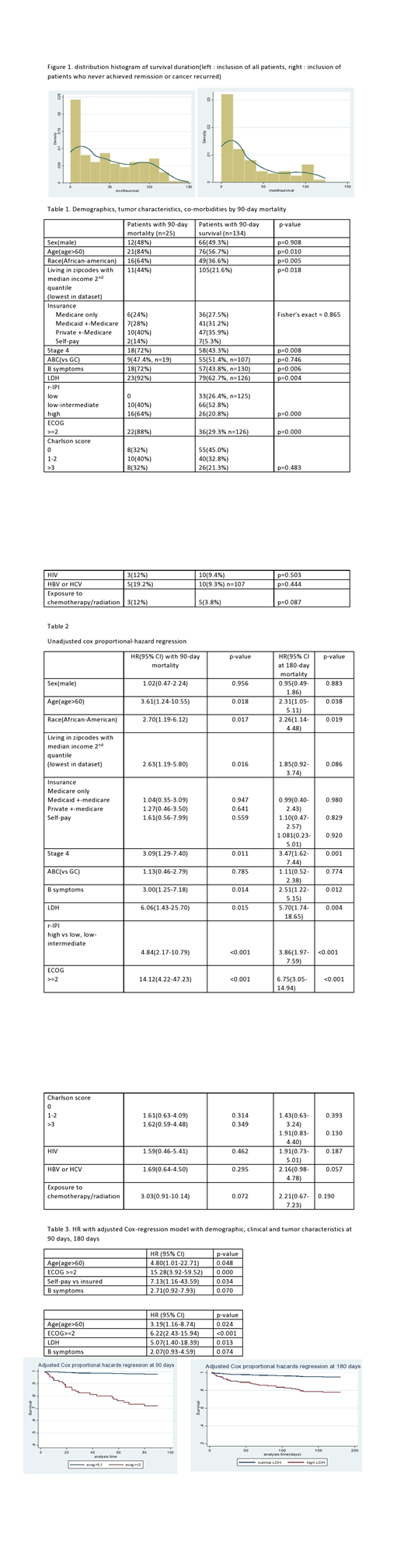
Among 159 patients, 25 and 34 patients (15.7% and 21.4%) had 90-day and 180-day mortality. The distribution of survival time was right skewed with more frequent death in early period(figure 1). Median survival of 90-day and 180-day mortality patients were 19 days and 33 days.
Among 25 patients with 90-day mortality, causes of death included rapid progression(48%), sepsis(32%), GI bleeding (32%), tumor lysis syndrome(24%), and withdrawal of care as not a treatment candidate with co-morbidities(16%). 56% of patients were discharged to comfort measure only. 16% patients underwent CPR. 25%(5 out of 25) in 90 day mortality group were started on Rituximab or other treatment measures compared to 100%(9 out of 9) between 90 -180-day mortality group(Chi-square<0.001).
Patients with 90-day mortality were more likely to be older age(over 60), African-American, a resident at low average income zip code, poor performance status, having stage 4 disease, B symptoms and high R-IPI score with statistical significance.
Adjusted Cox-proportional regression with demographic, tumor and clinical characteristics showed statistical significance both 90-days and 180-days with poor performance status with ECOG 2 or more(HR 15.28 and 6.22 in 90- and 180-day, both p-value <0.001) and older age(HR 4.18 and 3.19, p-value 0.048 and 0.024). Uninsured patients showed significantly high risk with HR 7.13(p-value 0.034) in 90-day mortality but no significance in 180-day mortality. High LDH was statistically significant only in 180-day mortality(HR 5.07, p-value 0.013). Other clinical characteristics including stage, R-IPI score, B symptoms lost significance after adjustment from uni-variate analysis.(table 2, 3)
Conclusion
Our study suggested poor performance status and old age is the most significant variables associated with early mortality than other characteristics. R-IPI or other tumor-associated factors have been known for predicting prognosis, which was supported by our previous study using same data, however this was not applied in association of early mortality after adjustment.
It is notable that two groups of patients with 90-day and with 180-day showed discrepancies in risk of mortality by being uninsured or having high LDH. Within early mortality group, there might be heterogeneity of clinical characteristics. For example, patients who not able to receive treatment or treatment was stopped with rapid progression or complications mostly died within 90 days, however patients who died between 90 days and 180 days all received Rituximab or other forms of treatment.
Many of our patients were old, African-American, residing in low-income area, advanced DLBCL with high ECOG. Only 56% of patients were discharged to hospice care or comfort measure only and 16% patient underwent CPR in patients with 90-day mortality while most of patients were not able to receive any treatment. Our study also implies the special need of addressing goals of care discussion in DLBCL patients early in the setting of underserved population.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal