

Introduction
The therapeutic options for diffuse large cell B cell lymphoma (DLBCL) patients (pts) that fail to respond/relapse after≥2 treatment regimens are limited. The SCHOLAR-1 study reported an overall response/ complete remission (ORR/CR) rates of 26%/ 7% with a median overall survival (OS) of 6.3 months in chemorefractory and early relapsing DLBCL pts.
Polatuzumab vedotin (Pola) is a conjugated antibody that delivers the microtubule inhibitor MMAE to CD79b-expressing cells. Polatuzumab administered in combination with Bendamustine-Rituximab (P-BR) has been recently approved by the FDA for pts with relapsed/refractory (R/R) DLBCL that failed to respond≥2 prior therapies.
The current study investigated the tolerability and efficacy of Pola mainly with BR, in DLBCL pts, treated through a compassionate program after failing ≥2 prior regimens.
Methods
Data of all pts with consecutive R/R DLBCL, treated with Pola-BR or Pola-R (2-8 cycles) in 11 Israeli centers between 6/2018 and -5/2019 were analyzed. Inclusion criteria for this study were: R/R DLBCL (denovo and transformed follicular lymphoma [t-FL]), age ≥ 18 years, ≥ 2 prior treatments. We evaluated pt characteristics, treatment details and toxicities, overall response and CR rates, progression free survival (PFS) and OS. Cox regression model was used to define factors affecting outcomes.
Results
34 patients- (denovo DLBCL, n=24 and t-FL, n=10 ⌈50% -non CGB and 50% - GCB type⌉) were included. Median age at Pola administration was 65.5 (range 60-72) years. Stage ≥3 disease was recorded in 88% and IPI ≥3 in 73.5%. Median prior lines was 3 (range 3-5); including anthracyclines and rituximab in 100% and cisplatin-based regimens in 91%. 32% relapsed after ASCT and 9% after CART infusion. 53% had primary refractory disease, 29% had refractory relapse and 18% had prior sensitive relapse. 22 pts received Pola-B, mostly with Rituximab (n=19), and 12 received Pola-R. In 5 pts, Pola-based regimen was used as a bridge for Allo SCT (all responded CR, n=4 and PR, n=1) and in 6 as a bridge to CARTs (all responded CR n=1, PR n=2, SD n=3). Median number of Pola B cycles was 3 (3-5) and median Pola-R cycles was 4 (3-6). Median B dose per cycle was 90 mg/m2 (45-90). GCSF was used in 47%. Early treatment discontinuation due to progressive disease (PD) occurred in 8 (23%) of the entire cohort: 23% of Pola-B pts and 25% of Pola-R pts.
Safety:
Hematological AEs grade 3-4, reported with Pola- B vs Pola-R were: neutropenia (45.5.% vs 33%), thrombocytopenia (25% vs 8%) and anemia (23% vs 17%). Infections were recorded in 41% and 36% of Pola-B pts and Pola-R respectively. Neutropenic fever was reported in 36% in Pola-B pts and none in Pola-R. Pulmonary infections were recorded in 33.3% and 27.3% of Pola-B and Pola-R pts respectively, resulting in death in one pt. Peripheral neuropathy occurred in 18% of Pola- B pts (grade ≤2) vs 8% with Pola -R. Hospitalization due to AEs was recorded in 41% of Pola-B vs 25% of Pola-R. Pola dose reduction due to AE was reported in 1 pt (8%) in the Pola-R.
Efficacy:
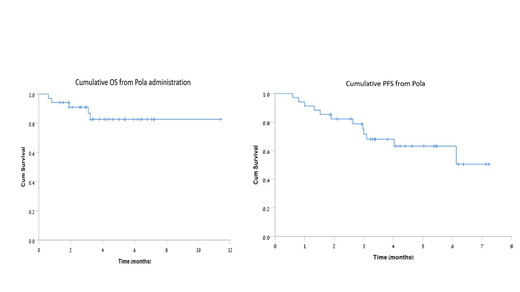
ORR for the entire cohort was 65%, including 38% CRs and 27% PRs. 12% pts attained SD and 23% experienced PD. ORR was higher in non-GCB than in GCB pts 80% vs 43% (p=0.036). Median follow up of the entire cohort from Pola administration was 4.4 months (range 0.6-11.4). 6 months projected OS and PFS were 83% and 63%, respectively.
Post Pola treatment in pts that failed to respond/Relapsed post pola:
8 patients had PD; 3 died from progression, 1-CART, 1-Allo SCT, 2-paliative care and 1-unknown. Additional 5 pts progressed during follow up; 4-CART and 1-palliative care. 1 patient continues Pola treatment after achieving SD.
Univariate analysis for factors predicting PFS and OS
GCB type (HR-1.816, P=0.055), Primary refractory vs relapsed disease (HR-1.507, p=0.049) and a higher number of prior lines since diagnosis (HR-1.35, p=0.079) tended to be associated with shorter time to progression. T-FL vs denovo DLBCL was associated with decreased OS (p=0.008).
Data of 60 patients, including pts treated recently, therefore, not evaluable at the time of abstract submission, would be presented at ASH.
Conclusions
The toxicity of Pola-based regimen was relatively low. Pola based treatment provided an encouraging PFS and OS in pts with R/R DLBCL that failed to respond ≥2 prior therapies, treated in a real-life setting. Primary refractory disease, higher number prior lines and t-FL vs denovo DLBCL were associated with inferior outcome.
Herishanu:Roche: Honoraria; AbbVie: Honoraria; Janssen: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal