

Classic Hodgkin's lymphoma (cHL) represents 95% of all Hodgkin lymphomas, and is responsible of 0.5% of all cancer types (Siegel, Miller & Jemal, 2016). In HIV positive patients, the incidence of cHL is high (5-20 fold). The use of combination antiretroviral therapy (CART) and CD4 count >200 cells/uL appears to increase the risk; nonetheless, the risk for developing cHL in HIV infected patients remains high, regardless of CD4 count. The median patients' age of HIV-associated classic Hodgkin's lymphoma (HIV-cHL) ranges from 40 to 49 years old, slightly higher than the age observed in general population. It is more common in men, and tends to manifest with extranodal disease (67% vs 32%), B-symptoms (77% vs 43%), and stage III or IV disease (82% vs 42%) (Shiels et al, 2014). Recent recommendations state that HIV-cHL should receive first-line ABVD chemotherapy treatment while continuing CART (Blanca et al, 2007)(Montoto et al, 2012).
To determine the prognosis of de novo advanced stage HIV-cHL and compare it with non-HIV-cHL, we designed an observational, descriptive study, including all HIV-cHL (WHO 2016 criteria) from August 2004 to December 2018, paired with a non-HIV-cHL group by clinical stage and gender.
Clinical features between positive and negative HIV groups were compared by standard statistical methods. Overall survival (OS) and relapse-free survival (RFS) were calculated by Kaplan-Meier methodology. Analysis for mortality predictors was performed with a univariate Cox regression model.
Data was collected from 21 patients with HIV-cHL, all male and with advanced clinical stage, and compared with 58 non-HIV-cHL patients with the same characteristics. The mean age observed was 42.9 (± 10.88) years in HIV-cHL, and 45.1 (± 17.56) years in non-HIV-cHL (p = 0.50).
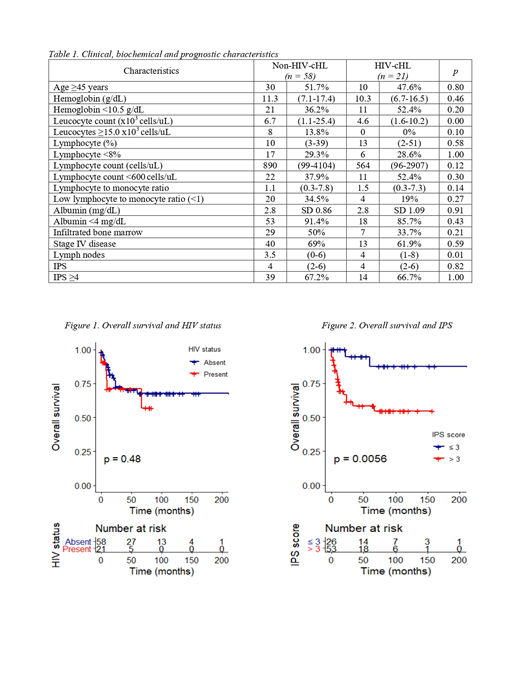
Among the clinical characteristics, the presence of B symptoms was documented in 85.7% of HIV-cHL, and in 91.4% of non-HIV-cHL (p = 0.43). Among biochemical characteristics in both groups, we observed a significantly lower leucocyte count in HIV-cHL (4.6x103 cells/uL) compared with non-HIV-cHL (6.7x103 cells/uL) (p = 0.02). In the monocyte line, we found that HIV-cHL had lower absolute counts (340 cells/uL) than non-HIV-cHL (708 cells/uL) (p = 0.01). A high IPS was reported in 66.7% of HIV-cHL, and in 67.2% of non-HIV-cHL (p = 1.00). The most common reported histologic subtype was mixed cellularity for both groups, with a prevalence of 38.1% and 38.9%, respectively (p = 0.25). The positivity for Epstein-Barr virus was tested in the biopsies of 18 HIV-cHL, and was 100%. Regarding HIV status in infected patients, a 40-month period was the median time between HIV and cHL diagnosis. The median CD4 cell count was 109 cells/uL. 90.5% of patients were treated with CART at time of cHL diagnosis.
Other clinical, biochemical and prognostic characteristics are in Table 1.
The median follow-up time for all patients was 31 months; the median follow-up time for HIV-cHL was 10 months, shorter than the median follow-up time for non-HIV-cHL (45 months) (p = 0.01). 85.7% of HIV-cHL and 96.6% of non-HIV-cHL received chemotherapy, with a median of 6 cycles (p = 0.11). Complete response (CR) was documented in 61.1% of HIV-cHL, and in 66.1% of non-HIV-cHL (p = 0.77). RFS was 36.5 months for all patients, being less for HIV-cHL (24 months) compared with non-HIV-cHL (51 months) (p = 0.03). The OS median at the time of last follow-up had not yet been reached in all patients (Figure 1).
The univariate analysis showed that age ≥45 years old and stage IV cHL are adverse prognostic factors (p = 0.02, p = 0.03, respectively). IPS ≥4 was an adverse outcome factor for mortality, with statistical significance (p = 0.01) (Figure 2). At last follow-up, 22 (27.8%) patients had died, 6 (28.6%) HIV-cHL and 16 (27.6%) non-HIV-cHL (p = 1.00).
Clinical, biochemical and prognostic variables, as well as treatment outcomes were similar between HIV-cHL and non-HIV-cHL. Although follow-up time in the HIV-cHL group is shorter, prognosis in terms of OS is similar. RFS is statistically different between both groups and is shorter in HIV-cHL, but as the OS in both groups remains similar, it is possible that rescue chemotherapy is effective in relapsed patients. There was no difference observed in the likelihood of achieving CR in both groups. IPS ≥4 and CR were independent prognostic factors for OS. IPS as an adverse factor and CR as a favorable one. Prognosis of advanced stage HIV-cHL is similar to non-HIV-cHL patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal