

Background. Ibrutinib became available for patients (pts) with relapsed/refractory (R/R) mantle cell lymphoma (MCL) in Russia in the end of 2015 based on the results of phase 2 study by M. Wang from MD Anderson Cancer Center (NEJM 2013, Blood 2015). However, pts in routine clinical practice tend to differ significantly from the patients selected for clinical trials, which may lead to poorer results in off study treated patients.
Aim. To assess efficacy and toxicity of ibrutinib monotherapy in pts with R/R MCL in routine community clinical practice outside of clinical trials.
Materials & Methods. We analyzed the charts of all pts with R/R MCL who started ibrutinib from April 2016 to July 2019 in 7 Moscow's hospitals. The following criteria were used to initiate ibrutinib monotherapy: the age > 18 years, confirmed MCL diagnosis with nuclear hyperexpression of cyclin D1 and/or presence of the t(11;14)(q13;q32); symptomatic relapse or failure to achieve at least PR with a prior regimen.
Poor physical status, pancytopenia grade 3-4, infectious complications (except for life-threatening conditions), blastoid variant and the number of previous treatment lines were not regarded as contraindications to ibrutinib therapy. Patients with CNS involvement were excluded from this analysis. Ibrutinib was administered once a day at a dose of 560 mg until progression or intolerable toxicity. Response to therapy was assessed every 2-3 months utilizing CT scan, PET/CT and bone marrow examination were required to confirm CR.
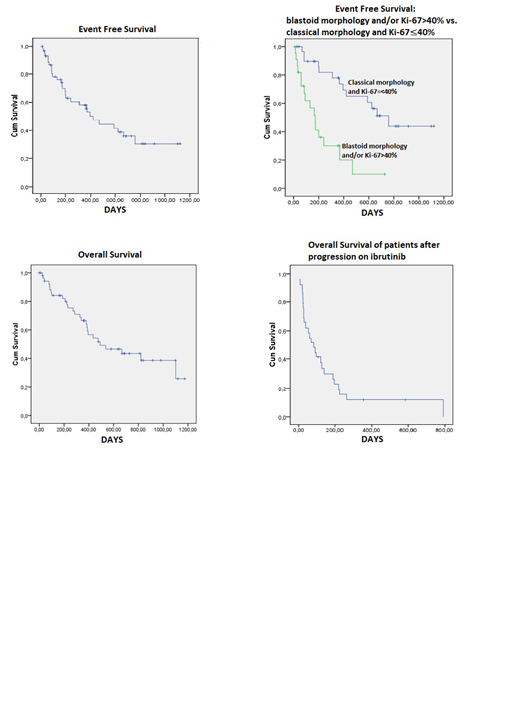
Results. 54 pts with R/R MCL received ibrutinib monotherapy between April 2016 and July 2019. 26 pts (48%) were refractory to a prior therapy. The median age was 68 years (range 40-81); 69% of pts were men; ECOG > 2 in 22% of pts. 15 pts (28%) underwent a repeated biopsy before starting ibrutinib. 23 pts (43%) had an aggressive variant of MCL: either blastoid morphology (13/54 at diagnosis and 5/54 after repeated biopsy) or classical morphology with Ki-67>40% (4/54 at diagnosis and 1/54 after repeated biopsy). The median number of previous treatment lines was 2 (1-11). The response was evaluated in 53/54 pts. ORR was 81%, CR rate was 30% in the whole group. Pts with aggressive variants of MCL (group 1) had ORR of 65%, CR rate of 7%. In the group with classical morphology and Ki-67≤40% (group 2) ORR and CR rates were 93% and 47%. 2 pts with a response to therapy stopped ibrutinib early on their own accord, without signs of toxicity above gr.1. The median EFS for all pts was 394 days (95% CI: 261-526). In group 1 the median EFS was 173 days (95% CI: 112-234), in the group 2 the median EFS was 759 days (95% CI: 521-996, p<0.0001). 27 pts (50%) died (25 deaths were MCL-related). The median OS for the entire population studied was 491 days (95% CI: 183-799). The median OS of pts after progression on ibrutinib was disappointingly short - 84 days (95% CI: 30-139). 21 pts (39%) remain on ibrutinib treatment for 10-1119 days (the median duration was 358 days).
The most common complications were myalgia and muscle cramps (60%, all gr.1-2), diarrhea (gr.1-2 in 58% and gr.3 in 4%); hemorrhagic complications (65%, all gr. 1-2); skin, nail toxicity and a rash (15%, all gr.1-2) and arrhythmia (9%). Infections were reported in 30% of pts (gr.3 in 6%). Skin/nails toxicity developed mainly after 6 months of ibrutinib intake. In 14 (26 %) pts ibrutinib treatment had to be adjusted (dose reduction or treatment interruption for 3-10 days) due to toxicity and planned surgeries. 4 pts (9%) required dose reduction from 560 to 420 mg. None of ibrutinib recipients had to completely discontinue ibrutinib therapy due to complications (with exception of 2 patients who stopped taking ibrutinib on their own). None of the patients received alloSCT.
Conclusion. These data on the use of ibrutinib in actual clinical practice are comparable with the results of international multicenter studies (PCYC-1104, SPARK, and RAY). Favorable toxicity profile and rather short time to antitumor response allow for ibrutinib administration in cases of poor performance status due to disease, low blood count, and even infectious complications.
Ibrutinib monotherapy results in the durable disease control in 93% of patients with non-blastoid MCL with the median EFS 25 months, but only 65% with blastoid type with the median EFS 6 months. However, some adverse effects are manifested not earlier than after 6-month treatment, which calls for continuous monitoring, especially when preparing for surgeries.
Vorobyev:AstraZeneca: Consultancy; Abbvie: Consultancy, Speakers Bureau; Roche: Consultancy, Speakers Bureau; Janssen: Consultancy, Speakers Bureau; Takeda: Consultancy, Speakers Bureau; Sanofi: Consultancy. Ptushkin:JSC GENERIUM: Research Funding; Alexion Pharmaceuticals, Inc:: Consultancy, Research Funding; Janssen: Consultancy; Roche: Consultancy; AbbVie: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal