

Background: Methotrexate-associated lymphoproliferative disorders (MTX-LPD) develops in patients with rheumatoid arthritis (RA) or other autoimmune disorders during low-dose MTX treatment. MTX-LPD includes wide variety disease spectrum, ranging from polymorphic proliferation to aggressive lymphoma. Although etiology of MTX-LPD has not been fully understood, approximately half of the MTX-LPD cases showed association with EB virus (EBV), suggesting that MTX treatment causes reduced immune response to EBV-positive cells, and results in MTX-LPD development.
Natural killer (NK) cells play important roles in eradicating tumor and virus-infected cells. NK cell function is modulated by multiple cell surface receptors, including Killer immunoglobulin-like receptor (KIR). There are multiple KIR genes (inhibitory or activated), which are various in number and/or composition among individuals, on chromosome 19q. Previous reports demonstrated that combination of KIR genes affects NK cell function, and is associated with the risk of development of certain types of cancers, viral infections and collagen disease. There is no report about the association of KIR genotype and MTX-LPD.
We consider that NK cells play a significant role in suppression of MTX-LPD development. In this study, we focused on examining genotype KIR and KIR-ligand (HLA class I).
Methods: We retrospectively analyzed 35 MTX-LPD cases diagnosed between 2009 and 2019. Genomic DNA was extracted from mononuclear cells that were isolated from the bone marrow or peripheral blood samples of patients with MTX-LPD. KIR genotypes were analyzed using the KIR genotyping sequence-specific primers kit. The variations of KIR content and haplotype and their relationship with progression to malignant lymphoma (ML) and response to chemotherapy were investigated. HLA was analyzed using PCR-Luminex assay. The frequency of each HLA allele and each combination was determined by referring to the data base of an HLA laboratory. Chi-squared (χ2) tests and Wilcoxon rank sum tests were used to test associations between the variables.
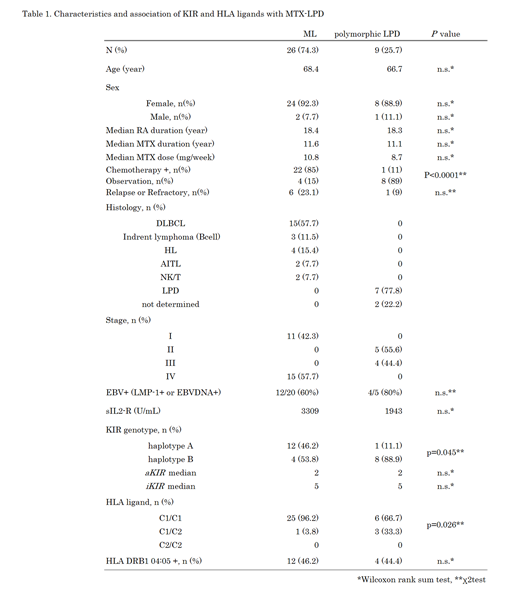
Results: Among the 35 patients, 25 were diagnosed with ML and 10 with polymorphic LPD. Diffuse large B cell lymphoma (DLBCL) was most common type in ML (57.7%). Table 1 showed characteristics of patients and summary of the results. All patients underwent MTX treatment for RA. The median duration of MTX administration at the time of MTX-LPD diagnosis is 11.5 years (range=0.8-27.2), and median MTX dose was 10mg/week (range=4-17.6). The duration and dose of MTX had no effect between ML and polymorphic LPD. Twenty-three patients required chemotherapy, and 12 patients had tumor regression after stopping MTX treatment. Relative patient populations requiring chemotherapy in ML or polymorphic LPD were 85% or 11%, respectively (P=0.0001). EBV-positive patients tended to regress tumors with MTX discontinuation alone (P=0.16).
In KIR genotype analysis, patterns of number and combination of the KIR genes are mainly classified as haplotype "A" containing multiple inhibitory KIR genes with a KIR 2DS4 (an activated KIR [aKIR]) and haplotype "B" (other than haplotype "A"). Patients were classified in haplotype A (13 cases, 37%) and haplotype B (22 cases, 63%), respectively. ML patients showed higher ratio in haplotype A (ML 46.2% vs LPD 11.1% P=0.045). There was no difference in number of aKIR or iKIR between ML and polymorphic LPD patients. In HLA Class I analyses, there was significant difference in frequencies of HLA-C haplotype between lymphoma and polymorphic LPD patients (P=0.026). Furthermore, HLA- C1 / C1 patients were more relapsed or refractory to chemotherapy than C1 / C2 patients (P = 0.17).
Conclusion: This is the first report showing clinical significance of KIR genotypes in MTX-LPD. Patients with haplotype A, a suppressive haplotype, seems to be at high risk for developing lymphomas that require chemotherapy during MTX treatment. HLA- C1/C1 patients are more likely to develop lymphomas that respond poorly to treatment, suggesting that the activity of NK cells may be lower because ligands can match with KIRs that are more restricted than C1/C2. Considering the potential NK functions with KIR genotype would improve the understanding of the prognosis and lead to prevention for MTX-LPD.
Hagiwara:Bristol Myers Squibb: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees. Harigai:Bristol Myers Squibb Co: Other: personal fees, Research Funding; Eisai Co: Other: personal fees, Research Funding; Ayumi Pharmaceutical Co: Other: personal fees, Research Funding; AbbVie Japan GK,: Other: personal fees, Research Funding; Eli Lilly Japan K.K: Other: personal fees; Kissei Pharmaceutical Co.: Other: personal fees; Teijin Pharma Ltd: Other: personal fees, Research Funding; Mitsubishi Tanabe Pharma Co: Research Funding; Nippon Kayaku Co.: Research Funding; Pfizer Japan Inc.: Other: personal fees; Chugai Pharmaceutical Co., Ltd.: Other: personal fees; Japan College of Rheumatology: Other: personal fees; Boehringer Ingelheim Japan, Inc: Other: personal fees; GlaxoSmithKline K.K: Other: personal fees; Oxford Immuotec,: Other: personal fees. Tanaka:Bristol-Myers Squibb: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal