

BACKGROUND
Patients with adverse cytogenetic or secondary AML (s-AML) have significantly worse outcomes and lower survival rates. In this high risk subgroup of patients, early consolidation with allogeneic hematopoietic stem cell transplantation (HSCT) in first complete remission (CR1) can improve results, especially in those who achieve negative measurable residual disease (MRD-). More effective treatments than standard 7+3 are needed. CLAG-M is a salvage regimen that has demonstrated high response rates with good tolerance, and seems to be promising in the upfront setting.
AIMS
To estimate CR and MRD- rates, overall survival (OS) and event free survival (EFS) in transplant eligible patients with high risk AML treated in our center.
To compare CR rate and transplant feasibility in CR1 with 7+3 vs. CLAG-M as induction treatment in s-AML.
PATIENTS AND METHODS
We analyzed adult patients (18-65 years old) with high risk AML (defined by adverse cytogenetic according to ELN2017 or s-AML) who were treated in our institution between 2010 and 2018. All patients were transplant eligible and had an available donor. Clinical information was collected from medical records. We evaluated CR1 and MRD- rates, EFS and OS. We also compared CR rates and HSCT feasibility in s-AML after treatment induction with CLAG-M and 7+3. The survival analysis was estimated with Kaplan-Meier method and the comparison between variables was performed through log-rank test.
RESULTS
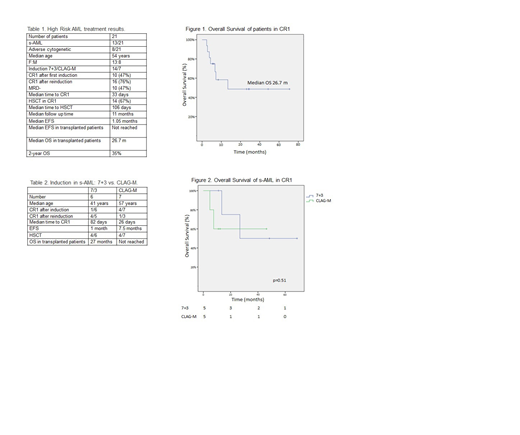
Twenty-one patients were included (13 s-AML and 8 with adverse cytogenetic). The median age at diagnosis was 54 years (21-64); 13 female/8 male. Out of 21 patients, 14 received 7+3 induction and 7 CLAG-M. The median follow-up time was 11 months (0.9-90.8), median EFS and OS for the whole group was 1.05 and 13.5 months, respectively. Two-year OS was 35%. CR1 was achieved in sixteen patients (76%), 10 of them MRD-. The median time to CR1 was 33 days, the median OS of these patients was 26.7 months (figure 1). Eleven patients (52%) were refractory to first induction, 10/14 in the 7+3 subgroup, and only 1/7 patients treated with CLAG-M. Six of them converted to CR after reinduction (5 with CLAG-M). Fourteen (67%) underwent HSCT in CR1. The median time to HSCT consolidation was 106 days. The median relapse free survival in transplanted patients has not been reached (Table 1).
Considering only s-AML, 6 patients received 7+3 and 7 CLAG-M. Median age in 7+3 subgroup was 41 vs. 57 years in CLAG-M. The median OS was 13.5 months. In the 7+3 cohort, only 1 achieved CR (16%); the other five received reinduction with CLAG-M, and 4 converted to CR1. The median time to CR1, EFS and OS were 82 days, 1 month and 26 months respectively. In contrast, 4 of the 7 patients (57%) that received CLAG-M achieved CR1, but only 1 of the 3 that were refractory could convert to CR. The median time to CR1 in patients treated with CLAG-M was 27 days, median EFS 7.5 months and median OS has not been reached (Figure 2). There were no statistically significant differences between the two treatment groups. Eight patients (62%) could be bridged to HSCT, 4 of each subgroup (Table 2).
CONCLUSIONS
Our results in this real life small cohort of high risk AML were similar to historical controls. In the s-AML subgroup, differences between 7+3 and CLAG-M were not statistically significant probably due to the low number of patients analyzed. However, patients who received CLAG-M required less cycles of treatment to achieved CR1, allowing HSCT rapidly in this selected population. Since most of the refractory patients to 7+3 responded to reinduction with CLAG-M, both groups had similar transplant rates.
According to our experience CLAG-M might be an attractive treatment option with high CR rates and acceptable safety profile. In this high risk AML population, two thirds of the patients were effectively "bridged" to HSCT with a 2-year OS rate of 35%.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal