

Background
Behçet's disease (BD) is a multisystem vasculitis characterized by exacerbations and remissions with unknown etiology. Males are more affected than females with the usual onset in the third decade. Vascular involvement can occur in up to 40% of cases of BD. BD is unique among the vasculitides that it may involve all sizes and types of vessels.
Objectives
1. To study the pattern of vascular involvement of Behçet's disease (BD) in the Saudi population; use of anticoagulation and its duration, thromboembolic, and major bleeding complications during anticoagulant therapy.
2. The effect of combined immunosuppression and anticoagulation treatment approach in reducing the risk of venous and arterial thromboembolism.
3. The role of vascular surgery for peripheral arterial and abdominal aortic aneurysms (AAA), and the role of immunosuppression in the treatment of pulmonary artery aneurysm (PAA) without the need for surgical intervention.
Methods
Twenty-three patients with confirmed vasculo-BD attending the thrombosis clinics at our tertiary care center between 2010 and 2015 were studied retrospectively and analyzed through descriptive statistics SPSS version 22.
Results
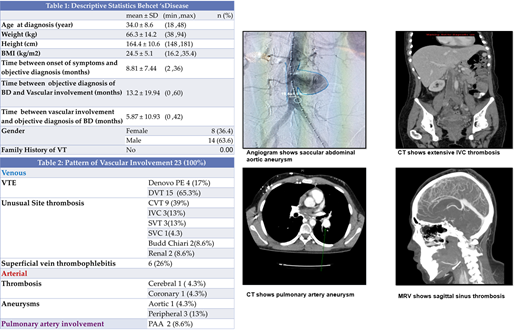
Demographics and pattern of vascular involvement are shown in tables 1 and 2. HLA-typing was performed for 13 patients, and HLA- B51 was positive in 7 (54%) patients tested. The acute phase reactants (ESR and CRP) were high in all 23 (100%). Hereditary and acquired thrombophilia workup was performed for all patients and only 1 (4.3%) was positive for antiphospholipid antibodies. Oral ulcers were present in all the patients, genital ulcers in 12 (52%), ocular involvement in 8 (35%), skin manifestations in 3 (13%), and arthritis in 1 (4.3%). Lower extremity vein thrombosis is the most frequent manifestation of Vasculo-BD in Saudi Arabia, followed by CVT, PAI, SVT/Budd-Chiari syndrome, IVC thrombosis, peripheral artery aneurysms, and AAA. Peripheral arterial and abdominal aortic aneurysms in 3 (13.6%), all of whom had successful vascular surgery for aneurysm repair. Inferior vena cava filter was inserted in 3 (13.6%). One patient was admitted to the intensive care unit with fulminant hepatic failure due to bilateral hepatic vein thrombosis and subsequently died.
The vascular thrombosis recurrence was in 11 patients (48%, all venous) despite adherence to the prescribed anticoagulant therapy and lack of any provocation. These patients were initially treated with anticoagulant monotherapy. After combining immunosuppressive therapy to the pre-existing anticoagulant therapy, none had thrombosis recurrence. There was a complete resolution of the two patients with PAA with mono-immunosuppressant therapy and no surgical intervention. The most commonly prescribed initiation anticoagulant therapy was low molecular weight heparin (87%).
Conclusion
BD with vascular involvement continues to pose a major diagnostic and therapeutic challenge to physicians due to the heterogeneity of the clinical presentation and lack of the diagnostic laboratory test. Therefore, we must have a low threshold for BD in any patient with vascular thrombosis or aneurysm. Combined immunosuppressive therapy is essential in suppressing and preventing the venous and arterial recurrence attacks.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal