

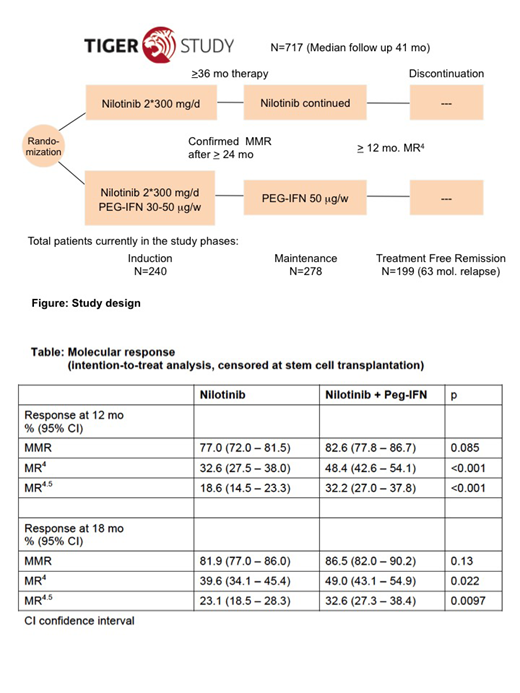
Introduction: The TIGER (CML V)-study* (NCT01657604) is a multicenter, randomized phase III trial to evaluate efficacy and tolerability of nilotinib (NIL) 2*300mg/d monotherapy vs NIL 2*300mg/d + pegylated interferon α2b (Peg-IFN) 30-50μg/week as first line therapy for chronic myeloid leukemia (CML) patients (pts) in chronic phase and discontinuation of therapy after Peg-IFN maintenance (Figure).
Methods: In August 2012, recruitment started with a pilot phase, aiming to validate the recommended dose of Peg-IFN. 25 pilot phase patients were treated with the combination of NIL 2*300 mg daily and Peg-IFN (30-50μg/week according to tolerability and commenced after ≥6 weeks NIL monotherapy). During the main phase of the study, 692 newly diagnosed pts were randomized between NIL 2*300 mg/d and NIL/Peg-IFN combination according to the outcome of the pilot phase.
Results: Within 5 years, a total of 717 pts (429 male; median age 51 years, range 18-85; 12.9% EUTOS high risk) were recruited from 109 sites in Germany, Switzerland, and the Czech Republic. 702 pts with typical BCR-ABL1 transcripts (97.9%) were eligible for molecular follow-up assessments according to the international scale (IS). Fifteen pts (2.1%) expressed atypical BCR-ABL1 transcripts. 692 pts were randomized after EUTOS risk stratification to receive NIL monotherapy (n=353) or NIL/PEG-IFN combination therapy (n=339). Median observation time since recruitment was 41 months. Up to now, 477 pts concluded the induction phase by achieving a confirmed major molecular response, MMR (BCR-ABL1 transcript levels ≤0.1% IS, which qualified for entering the maintenance phase of the study using NIL or Peg-IFN monotherapy. During the maintenance phase, 199 pts achieved or sustained MR4 (BCR-ABL1 ≤0.01% IS) for at least one year and then discontinued all therapy.
While the rate of MMR at 12 and 18 mo - the first primary endpoint of the study - was not different between the treatment arms, adding Peg-IFN to upfront NIL significantly improved rates of MR4 and MR4.5, BCR-ABL1 ≤0.0032% IS) (Table). In competing risk analysis, median time to MMR was 5.7 vs 5.4 mo, to MR4 20.9 vs 12.5 mo, and to MR4.5 33.8 vs 23.2 mo for NIL vs NIL/Peg-IFN, respectively.
After NIL discontinuation, during Peg-IFN maintenance therapy, rate of molecular recurrence (BCR-ABL1 >1% IS) after 18 mo was 28%. From 199 pts who discontinued all therapy, 63 experienced a molecular relapse (BCR-ABL1 >0.1%). Relapse free survival by 18 mo after treatment discontinuation was 61% in the total cohort. By protocol, it is too early to assign relapse rates to the randomized treatment arm.
Frequencies of adverse events after 24 mo of therapy were 90 and 92% (grade 1-5) and 36 and 42% (grade 3-5) for NIL vs NIL/Peg-IFN, respectively. Adverse events of special interest (all grades) were fatigue in 34.6 vs 40.4%, thrombocytopenia in 13.3 vs 18.9% and elevation of the alanin aminotransferase (ALAT) in 11.0 vs 18.9% of pts in the NIL vs NIL/Peg-IFN arms, respectively. Fifteen pts (2.1%) progressed to accelerated phase or blast crisis; 22 pts (3.1%) received an allogeneic stem cell transplantation, 10 of them after disease progression. In total, 22 pts (3.1%) died, 16 during the induction phase, 4 in the maintenance phase and 2 in treatment free remission. Four deaths were related to CML, 3 to vascular complications.
Conclusions: This per protocol interim analysis demonstrates feasibility of the first-line treatment with NIL 2*300 mg/d combined with PEG-IFN 30-50 μg/week. Peg-IFN, when added upfront to NIL further increases the rates of MR4 and MR4.5, which may translate into higher rates oftreatment free remission.
*The study is being conducted on behalf of the German CML Study Group, the Swiss Group for Clinical Cancer Research (SAKK) and the East German Study Group on Hematology and Oncology (OSHO).
Hochhaus:Pfizer: Research Funding; Novartis: Research Funding; BMS: Research Funding; Incyte: Research Funding; MSD: Research Funding. Burchert:Novartis: Research Funding. Saussele:Novartis: Honoraria, Research Funding; Incyte: Honoraria, Research Funding; BMS: Honoraria, Research Funding; Pfizer: Honoraria. Baerlocher:Novartis: Research Funding. Brümmendorf:Janssen: Consultancy; Ariad: Consultancy; University Hospital of the RWTH Aachen: Employment; Pfizer: Consultancy, Research Funding; Merck: Consultancy; Novartis: Consultancy, Research Funding. La Rosée:Novartis: Research Funding; Bristol-Myers-Squibb: Consultancy, Other: Travel support, Speakers Bureau. Heim:Novartis: Research Funding. Krause:Siemens: Research Funding; Takeda: Honoraria; MSD: Honoraria; Gilead: Other: travel; Celgene Corporation: Other: Travel. le Coutre:Bristol-Myers Squibb: Honoraria, Speakers Bureau; Incyte: Honoraria, Speakers Bureau; Novartis: Honoraria, Speakers Bureau; Pfizer: Honoraria, Speakers Bureau. Niederwieser:Daichii: Speakers Bureau; Cellectis: Consultancy. Lange:Novartis: Research Funding. Fabarius:Novartis: Research Funding. Hänel:Novartis: Honoraria; Amgen: Honoraria; Takeda: Other: advisory board; Celgene: Other: advisory board; Roche: Honoraria. Stegelmann:Novartis: Consultancy, Honoraria; Incyte: Consultancy, Honoraria. Mayer:AOP Orphan Pharmaceuticals AG: Research Funding. Hasford:Novartis: Research Funding. Hehlmann:Novartis: Research Funding. Ernst:Novartis: Research Funding.
Combination of Nilotinib and PEG-IFN alpha is being tested is off-label and being tested in the TIGER study.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal