

A 45 yo woman with a medical history of common variable immunodifficiency (CVID) was referred for a bleeding disorder. The bleeding was manifested daily with ecchymosis and epistaxis, but prior to the visit, she developed a lower pelvic mass that was a massive hematoma requiring transfusion. In 2011 she had a splenectomy for thrombocytopenia. After splenectomy, her liver enlarged and one year prior to being seen, she was started on everolimus as part of a protocol to reduce her liver size.
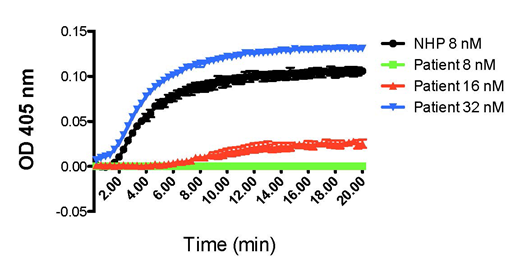
Bleeding started 3-6 months after starting everolimus treatment, first manifesting with recurrent lower gastrointestinal hemorrhage. In 2011 she had normal PT and aPTT. At the present time her PT remains normal at 11.43+0.67 (Mean+SD) (normal 9.7-12.7 sec); but her aPTT is abnormal at 43+6.1 (normal 28-38 sec); clottable fibrinogen (Fb) 305+72 (normal 200-400 mg/dl); Fb antigen, 428+115 mg/dl (normal 196-441); ratio of clottable Fb/Fb antigen = 0.71+ 0.06; reptilase time 20+2.2 (normal 14-23 sec); and her thrombin time of 19+1.6 is prolonged (normal 10-16 sec). Blood coagulation factors XI, IX, VIII, VII, X, V, II, and XIII were normal. Further, she did not have excess alpha-1-antitrypin, antithrombin, or protein C to suppress thrombin generation. On a 1:1 mixing study of normal plasma:patient plasma, her thrombin time corrected to normal. Since the patient had an abnormal thrombin time with serious, spontaneous, clinical bleeding with a normal reptilase time, we postulated a fibrin polymerization defect. On a fibrin polymerization assay, the patient required 4-fold greater amounts (32 nM vs 8 nM) of human alpha thrombin to achieve complete fibrin polymerization (See Figure 1 below). On complete fibrinogen sequencing, the patient was found to have a pathologic mutation [Fb gamma chain exon 3, 124G>A, Gly42Ser (Gly16Ser in the mature gamma chain without the signal peptide)]. This defect had been previously described as Fibrinogen Krakow III (Pietrys D et al. Thromb Haemost. 2011;106:558-60). However, neither parent of the patient has a bleeding disorder. Sequencings of her parents' Fb gamma chains show no mutation.
Since first being seen, the patient had a serious bleed into her right sacral plexus leaving her with a permanent foot drop. We managed her bleeding with cryoprecipitate replacement acutely and oral tranexamic acid as an outpatient. Everolimus is an mTor inhibitor which is a regulator of protein synthesis. We postulated that everolimus therapy produced the acquired abnormal Fb gamma synthesis, producing the fibrin polymerization defect associated with bleeding. Upon urging, the patient stopped everolimus therapy and has not had a major bleeding incident in 8 months although the abnormal thrombin time persists.
Wolberg:Novo Nordisk: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal