

Introduction
Diffuse large B-Cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma (NHL). Up to one third of patients relapse or fail to achieve complete remission, with poor prognosis. and low response rates to salvage treatments. Early identification of patients unlikely to be cured with R-CHOP might improve their chance of cure and quality of life. Interim [18F]FDG PET (I-PET) measures the pattern of response during treatment, which might add important prognostic value. These measures could be used for I-PET guided treatment for both patients with a good response and patients with a poor response. At this moment it is unclear what the influence of timing and PET positivity criteria is on the prognostic value of I-PET. Therefore, the aim of this individual patient data (IPD) meta-analysis was to determine the optimal timing and optimal PET positivity criteria for I-PET to predict response in DLBCL patients.
Methods
Individual patient data from 1977 de novo DLBCL patients were obtained from the PETRA database (www.petralymphoma.org). These patients had been enrolled in 9 clinical studies and treated with R-CHOP14, R-CHOP21 or DA-EPOCH-R. All patients had an I-PET following one to four cycles of therapy. Progression free survival (PFS) was the primary endpoint. We used the Deauville score (DS) as a visual assessment of the I-PET with two different cut-offs for PET-positivity: DS 4-5 positive and DS 5 positive. Relative reductions (Δ) of Standardized Uptake Values (SUV) were used for semi-quantitative scoring of I-PET. A cut-off of 66% reduction was used for I-PET scans after 1,2 or 3 cycles and a cut-off of 70% was used for I-PET after 4 cycles. DS were available for 1828 patients and ΔSUV data for 1632 patients. Multilevel Cox proportional hazards models were used to study the effects of timing and PET positivity criteria on 2-year PFS, with I-PET after 2 cycles as reference.
Results
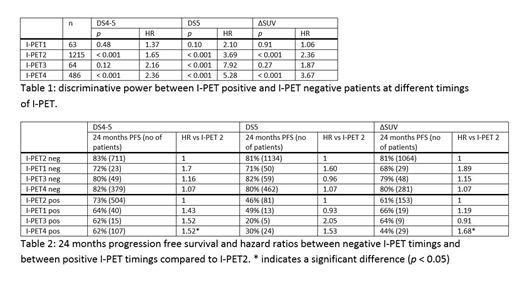
After correction for Ann Arbor stage and age, there were no significant differences in PFS between the 9 studies. I-PET1 was not able to significantly discriminate between responders and non-responders. I-PET2 and I-PET4 were able to significantly discriminate responders and non-responders, with higher hazard ratios (HR) for I-PET4. HR were 1.65 and 2.36 for DS4-5 positive, 3.69 and 5.28 for DS5 positive and 2.36 and 3.67 for ΔSUV criteria for I-PET2 and I-PET4 respectively. I-PET3 was able to significantly discriminate responders and non-responders only for DS5 positive criteria (HR: 7.92) (Table 1). However, there were few patients with I-PET1 and I-PET3 scans. Regarding I-PET negative patients, there were no significant differences in PFS using any of the response criteria at the 4 timepoints assessed. Regarding I-PET positive patients, there was a significantly lower PFS at I-PET4 than at I-PET2 , using the DS4-5 positive criteria (p = 0.009, HR = 1.52 (95% BI 1.11 - 2.09)) and ΔSUV criteria (p = 0.05, HR = 1.68 (95%BI 1.00-2.82)) but no other significant differences using other criteria or timepoints (Table 2).
Conclusions
I-PET is able to significantly discriminate between responding and non-responding patients after 2, 3 or 4 cycles of chemotherapy. The optimal timing to identify responders is after 2 cycles, as there is no significant increase in survival at later times, regardless of PET criteria. As the PFS of I-PET4 positive patients is significantly lower than that of I-PET2 patients, I-PET4 might be the optimal timing to identify non-responders. We suggest to perform an I-PET4 scan to identify poor-responding patients. The worst prognostic subgroup is best identified using the DS 5 positive or ΔSUV criteria. Based on these data, I-PET could be used to design response adapted trials for patients with good and poor responses respectively.
Barrington:Roche: Honoraria, Research Funding, Speakers Bureau; Celgene: Research Funding; Amgen: Research Funding; Bristol Myers Squibb: Research Funding; Takeda: Honoraria, Speakers Bureau. Dührsen:Alexion: Honoraria; Roche: Honoraria, Research Funding; AbbVie: Consultancy, Honoraria; Gilead: Consultancy, Honoraria; Janssen: Honoraria; Teva: Honoraria; CPT: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Amgen: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Honoraria; Celgene: Research Funding. Hüttmann:University Hospital Essen: Employment; Takeda: Honoraria; Gilead: Honoraria. Zucca:Janssen: Research Funding; AstraZenaca: Research Funding; Kite, A Gilead Company: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celltrion Helathcare: Membership on an entity's Board of Directors or advisory committees; Merck: Research Funding; Roche: Membership on an entity's Board of Directors or advisory committees, Other: Travel Grant, Research Funding; Abbvie: Other: Travel Grant. Higley:FNIH: Research Funding; CCS associates: Employment; NCIS/Leidos: Research Funding. Hutchings:Genmab: Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Research Funding; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel Expenses, Research Funding; Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees, Other: Travel Expenses, Research Funding; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel Expenses, Research Funding. Lugtenburg:Celgene: Consultancy, Honoraria; Genmab: Consultancy, Honoraria; Janssen Cilag: Honoraria; Servier: Consultancy, Honoraria, Research Funding; BMS: Consultancy; Roche: Consultancy, Honoraria, Research Funding, Speakers Bureau; Takeda: Consultancy, Honoraria, Research Funding. Zijlstra:Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Gilead: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal