

Introduction: Individuals with sickle cell disease (SCD) experience both acute vaso-occlusive pain (VOC) and chronic pain, both primarily treated with opioids. However, opioids only address the sensory dimension of pain and repeated use of opioids can cause short and long-term side effects such as respiratory system depression, increased risk of cardiovascular events, and hyperalgesia. Non-pharmacologic approaches to the management of acute and chronic SCD pain, such as cognitive behavioral therapy, biofeedback, acupuncture, hypnosis, and megavitamins, have shown positive effects for pain management and may reduce opioid use. Among non-pharmacologic pain management methods, aquatic therapy has been underutilized and understudied in patients with SCD, despite showing benefits for pain management and quality of life in adults with musculoskeletal conditions. At Vidant Medical Center, aquatic therapy has been introduced for patients with SCD in 2015 and has been increasingly used since then. To describe the use of aquatic therapy and outcomes in pediatric patients with SCD, we retrospectively evaluated the use of this therapy at Vidant Medical Center among children hospitalized for acute VOC pain.
Methods: The study was approved by the Institutional Review Board at East Carolina University. Children with SCD between 7-18 years of age at the time of admission for acute VOC pain between the years 2015-2018 were included in the analysis. During the review period, orders for aquatic therapy were placed at the provider's discretion. Our primary outcome was utilization of aquatic therapy during a given hospitalization, determined by retrospective query of the electronic medical record (EMR). Secondary outcomes include length of stay and time to readmission for VOC. Covariates were assessed at the time of the index admission included age, sex, and insurance coverage. Mixed-effects logistic or Poisson regression models were fitted to account for multiple hospitalizations per patient.
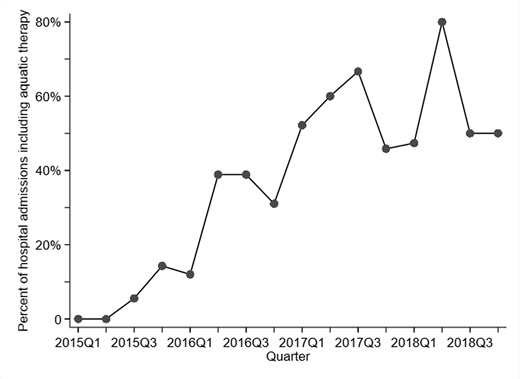
Results: The analysis included 316 hospitalizations of 87 patients (48% female; median age at the earliest hospitalization, 11 years). The median duration of hospital admissions was 4 days (interquartile range [IQR]: 3, 7). Aquatic therapy was used in 38% of admissions, with a trend of increasing use during the study period (Figure 1). On multivariable logistic regression analysis of aquatic use during a given admission, characteristics associated with greater likelihood of aquatic therapy use included older age and more recent year of admission. Aquatic therapy was associated with 69% longer hospital stays, although this may be related to availability of aquatic therapy services. Among 52 patients with multiple admissions, use of aquatic therapy during a given admission was associated with 26% more days between hospitalizations (incidence rate ratio = 1.26; 95% CI: 1.21, 1.31; p=<0.001).
Conclusion: Research into the use of non-pharmacologic pain management strategies for sickle cell disease has recently increased in order to better address the multidimensional aspects of pain. Of these management strategies, aquatic therapy has been very underutilized and under researched. Analysis of the utilization of aquatic therapy in our institution showed improved use over the last 3 years as well as increased duration between hospitalizations after the use of aquatic therapy. These positive results point towards the need for more research into other outcome measures derived from the use of aquatic therapy in pain management of pediatric SCD patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal