

Objectives: Distinguishing between acute presentations of osteomyelitis (OM) and vaso-occlusive crisis (VOC) bone infarction in children with sickle cell disease (SCD) remains challenging for clinicians, particularly in culture-negative cases. VOC and osteomyelitis have a very similar presentation in the acute stage, and both are associated with a rise in C-reactive protein (CRP) level and erythrocyte sedimentation rate (ESR). The gold standard to diagnose osteomyelitis is obtaining a positive blood culture and bone/joint biopsy which is invasive and not frequently done. Standard magnetic resonance imaging (MRI) with fat suppression sequencing (subtraction technique) may help to confirm osteomyelitis in SCD patients; however, this is frequently not done in a timely manner and is associated with false positive and false negative results. The objective of this study is to assess the discriminative impact of baseline variable and build a score to assess the diagnosis of osteomyelitis in pediatric patients with SCD.
Methods: A retrospective study of all patients with SCD, aged 1 to 18 years old with suspected osteomyelitis. The study covered a period of over 4 years (January 2015- June 2019) at Sultan Qaboos University Hospital, which is the main tertiary care and referral facility in Oman. All the patients were subjected to a complete clinical assessment, laboratory blood tests including, CBC, CRP, blood and aspirated fluid (if applicable) culture, and standard MRI with fat suppression sequencing of the affected bone. A clinical and laboratory score was designed to test whether it can help to prove or disprove the diagnosis in likely cases (Table 1).
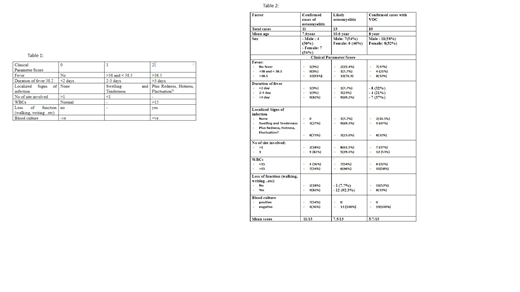
Results: A total of 43 patients fulfilled the inclusion criteria. Their mean age was 8.7 years +/-3.4. Male to female ratio was 1.87:1. All patients have been initiated on antibiotic therapy as osteomyelitis based on the clinical suspicion and MRI findings. The mean score in the 11 patients with confirmed osteomyelitis was 11/13. Thirteen patients were classified as likely osteomyelitis. Their mean score was 7.5/13. Seventeen patients were confirmed to have VOC by the clinical course (fast resolution of fever, local signs of inflammation and the drop in inflammatory markers). Their mean score was 5.7/13 (Table 2).
Conclusion: Differentiating VOC from osteomyelitis in children with SCD who present with fever and bone pain is a difficult task. Our proposed score assigned different mean score to different clinical entity (confirmed OM vs. likely OM vs. VOC). This score may assist clinicians to differentiate these entities. A larger prospective study is needed to confirm and validate the score.
Tbaileh:Sultan Qaboos University Hospital: Other: Data Collection, Data Input , Discussion of data with my seniors. Al-Khabori:Roche: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; SOBI: Honoraria; AstraZeneca: Honoraria; NovoNardisk: Membership on an entity's Board of Directors or advisory committees; Servier: Membership on an entity's Board of Directors or advisory committees; Shire (Takeda): Membership on an entity's Board of Directors or advisory committees. Wali:Sultan Qaboos University Hospital: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal